Downloaded 113 times
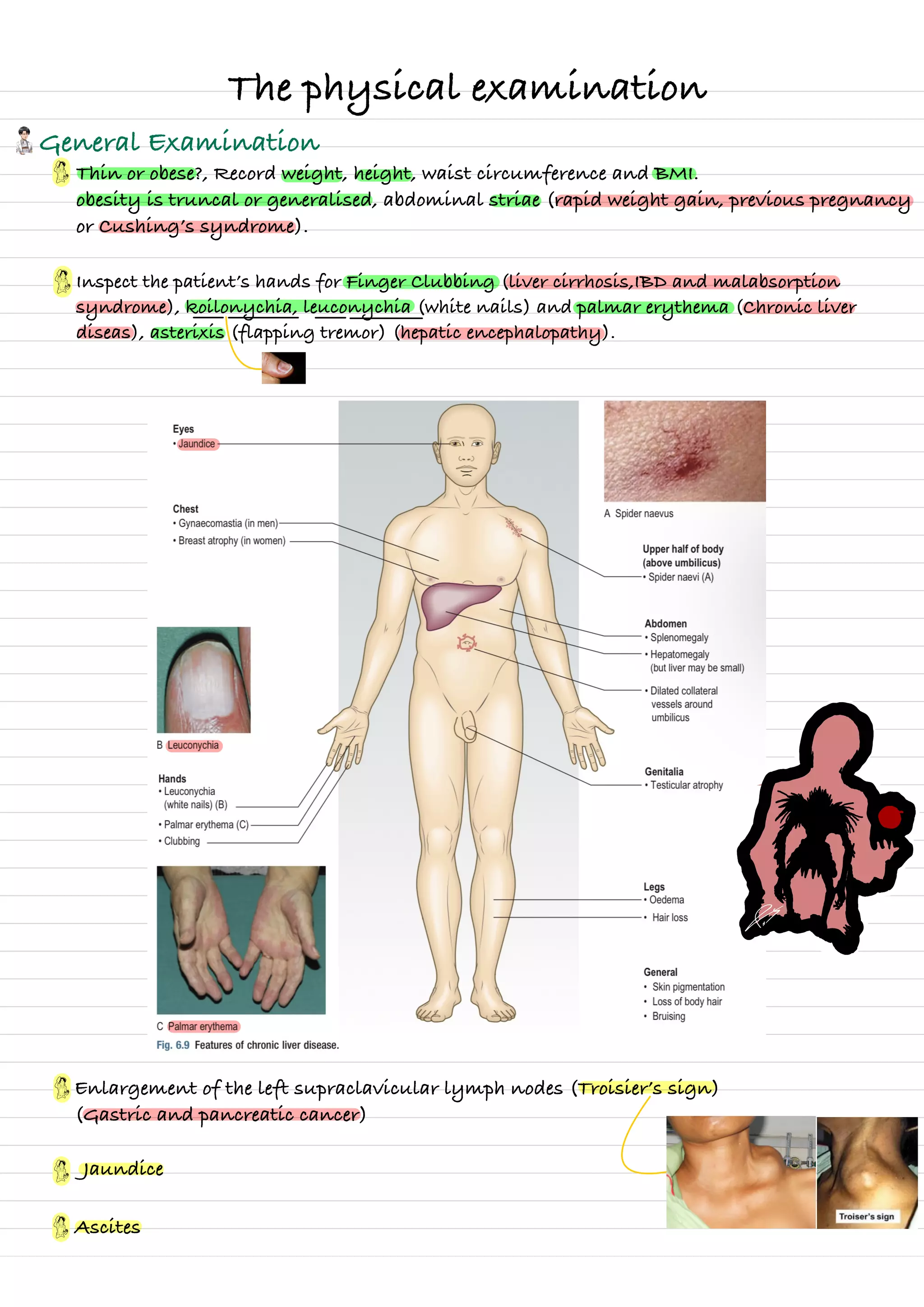



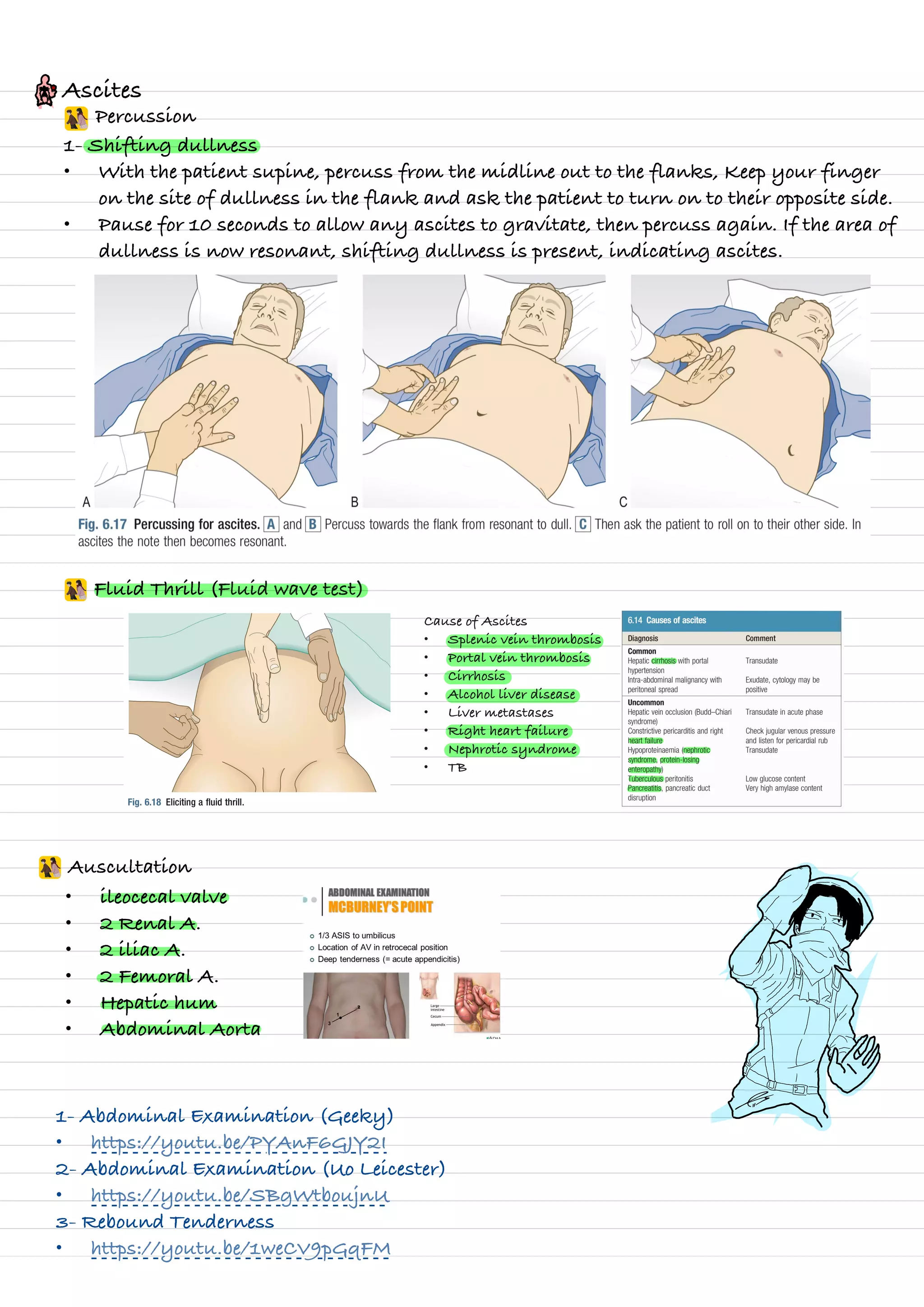

The document provides guidance on performing a physical examination of the abdomen. It describes inspecting the abdomen to check for distention, striae, pulsations, scars or masses. Palpation involves checking for tenderness, enlarged organs, masses, and shifting dullness over the liver and spleen. Percussion is used to evaluate the borders of the liver and spleen. Auscultation listens for bowel sounds and vascular sounds over arteries. The examination evaluates for signs of conditions like ascites, hepatomegaly, splenomegaly, and their underlying causes.























































































