Download to read offline




















![• Hovelius B, Mårdh PA. Staphylococcus saprophyticus as a common cause of urinary tract infections. Reviews of infectious diseases. 1984 May 1;6(3):328-37.
• Ioannou P, Mavrikaki V, Kofteridis DP. Roseomonas species infections in humans: a systematic review. Journal of Chemotherapy. 2020 Jul 3;32(5):226-36.
• Ionescu MI, Neagoe DȘ, Crăciun AM, Moldovan OT. The Gram-negative bacilli isolated from caves—Sphingomonas paucimobilis and Hafnia alvei and a review of
their involvement in human infections. International journal of environmental research and public health. 2022 Feb 17;19(4):2324.
• Jain S, Nagarjuna D, Gaind R, Chopra S, Debata PK, Dawar R, Sardana R, Yadav M. Escherichia vulneris: an unusual cause of complicated diarrhoea and sepsis in
an infant. A case report and review of literature. New microbes and new infections. 2016 Sep 1;13:83-6.
• Jamiu AT, Albertyn J, Sebolai OM, Pohl CH. Update on Candida krusei, a potential multidrug-resistant pathogen. Medical mycology. 2021 Jan;59(1):14-30.
• Jiang S, Li M, Fu T et al. (2020). Clinical characteristics of infections caused by Streptococcus sanginosus group. Au Sci Rep. 10(1):9032.39.
• Kawalec, A.; Zwoli´nska, D. Emerging role of microbiome in the prevention of urinary tract infections in children. Int. J. Mol. Sci. 2022, 23, 870. https://doi.org/
10.3390/ijms23020870
• Kirk F, Mashicharan M, Braddick M, Saxena P. Staphylococcus hyicus, a novel pathogen causing destructive infective endocarditis requiring mitral annular
reconstruction. JTCVS Tech. 2022 Apr 15;13:70-73. doi: 10.1016/j.xjtc.2022.03.008.
• Kotzekidou P. Geobacillus stearothermophilus (Formerly Bacillus stearothermophilus), Editor(s): Carl A. Batt, Mary Lou Tortorello,Encyclopedia of Food
Microbiology (Second Edition),Academic Press,2014,Pages 129-134, ISBN 9780123847331, https://doi.org/10.1016/B978-0-12-384730-0.00020-3.
• Liu J, Wang R, Fang M. Clinical and drug resistance characteristics of Providencia stuartii infections in 76 patients. Journal of International Medical Research. 2020
Oct;48(10):0300060520962296.
• Liu Y, Zai X, Weng G, Ma X, Deng D. Brevibacillus laterosporus: A probiotic with important applications in crop and animal production. Microorganisms. 2024 Mar
12;12(3):564.
• Lynch JP 3rd, Clark NM, Zhanel GG. Infections Due to Acinetobacter baumannii-calcoaceticus Complex: Escalation of antimicrobial resistance and evolving
treatment options. Semin Respir Crit Care Med. 2022 Feb;43(1):97-124. doi: 10.1055/s-0041-1741019.
• Mahdhi A, Kamoun F, Messina C, Santulli A, Bakhrouf A. Probiotic properties of Brevibacillus brevis and its influence on sea bass (Dicentrarchus labrax) larval
rearing. African Journal of Microbiology Research. 2012 Sep 13;6(35):6487-95.
• Mironov AIu, Savitskaia KI, Vorob'ev AA. Uslovno-patogennye mikroorganizmy pri zabolevaniiakh mochepolovykh puteĭ [Opportunistic microorganisms in urinary
tract diseases]. Vestn Ross Akad Med Nauk. 2001;(2):7-11.
• Morrison AJ Jr, Boyce K 4th. Peritonitis caused by Alcaligenes denitrificans subsp. xylosoxydans: case report and review of the literature. J Clin Microbiol. 1986
Nov;24(5):879-81. doi: 10.1128/jcm.24.5.879-881.1986.
• Mullineaux-Sanders C, Carson D, Hopkins EG, Glegola-Madejska I, Escobar-Zepeda A, Browne HP, Lawley TD, Frankel G. Citrobacter amalonaticus Inhibits the
Growth of Citrobacter rodentium in the Gut Lumen. Mbio. 2021 Oct 26;12(5):10-128.
• Naveed M, Sheraz M, Amin A, Waseem M, Aziz T, Khan AA, Ghani M, Shahzad M, Alruways MW, Dablool AS, Elazzazy AM. Designing a novel peptide-based
multi-epitope vaccine to evoke a robust immune response against pathogenic multidrug-resistant Providencia heimbachae. Vaccines. 2022 Aug 11;10(8):1300.
• Numberger D, Siebert U, Valentin Weigand P. Survival and adaptation of Streptococcus phocae in host environments. Plos one. 2024 Jan 30;19(1):e0296368.
• Pessoa RB, Oliveira WF, Correia MT, Fontes A, Coelho LC. Aeromonas and human health disorders: clinical approaches. Frontiers in microbiology. 2022 May
31;13:868890.
Epidemiology, ICAR-IVRI, Izatnagar](https://image.slidesharecdn.com/acomparativestudyonuroculturomeantimicrobialsusceptibilityinapparentlyhealthyandurinarytractinfected-240701045021-f89bd9ae/75/A-comparative-study-on-uroculturome-antimicrobial-susceptibility-in-apparently-healthy-and-urinary-tract-infected-humans-pptx-23-2048.jpg)



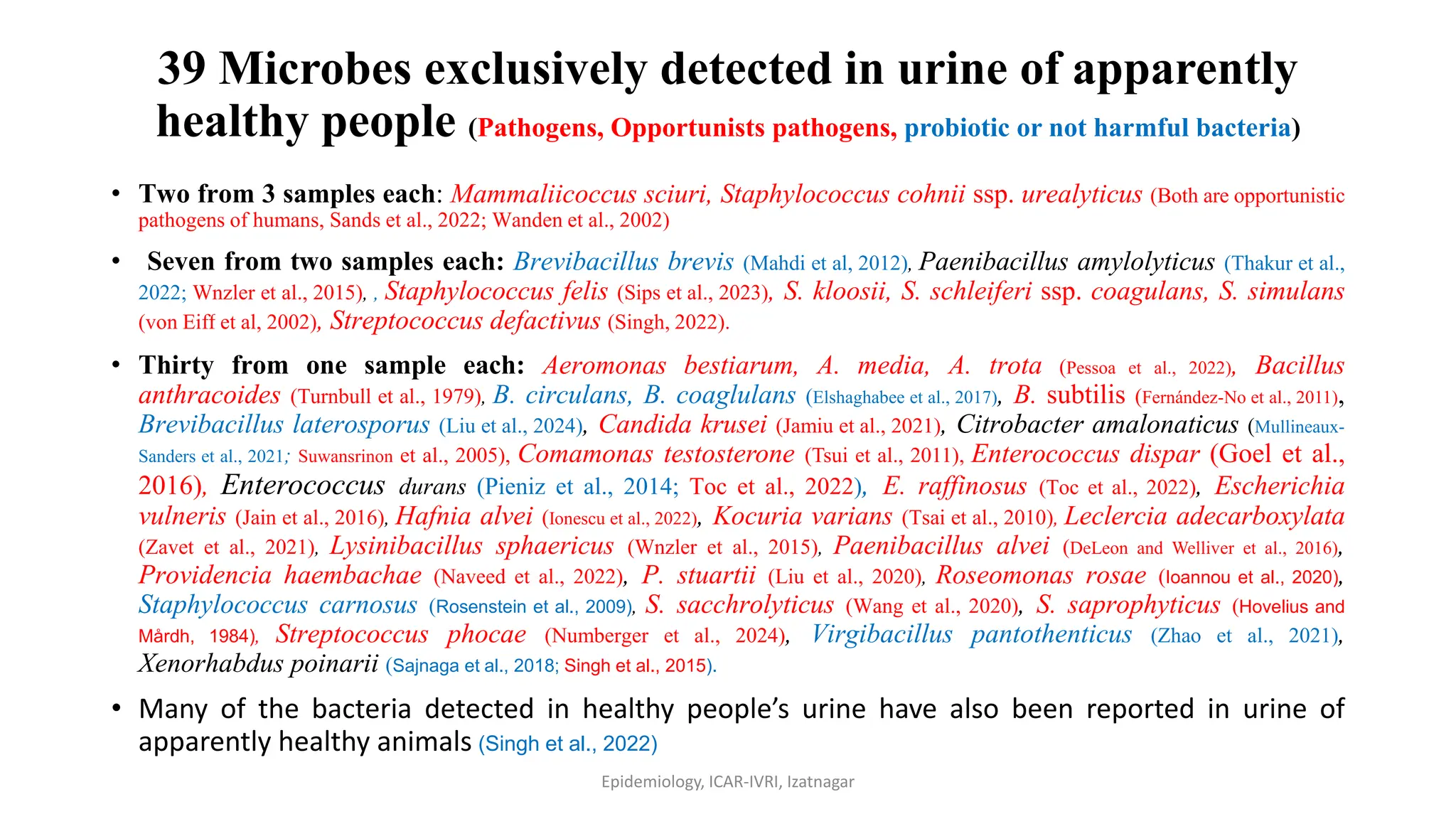
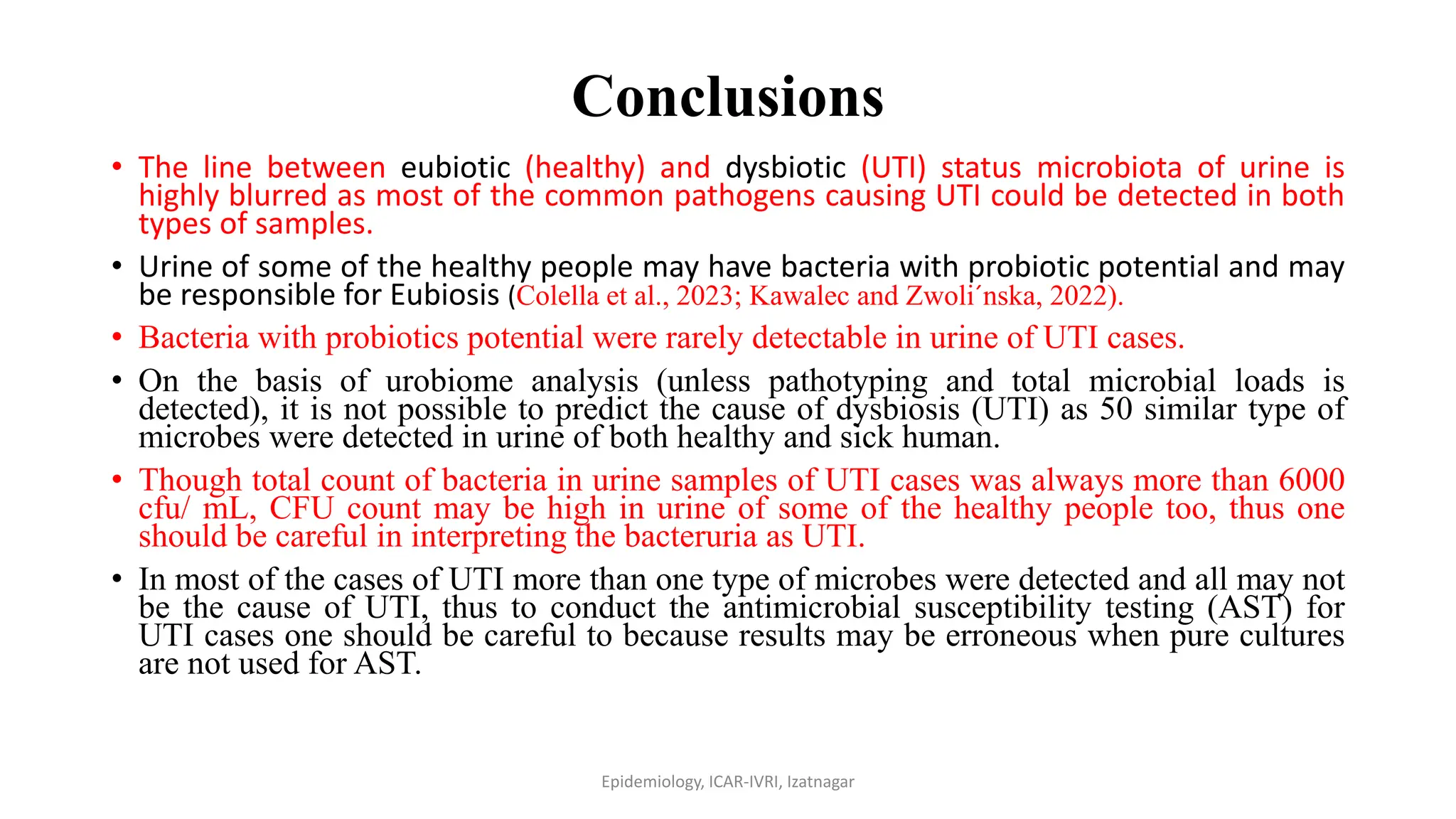
This study investigates the uroculturome and antimicrobial susceptibility of microbial communities in urine from 128 healthy individuals and 161 patients with urinary tract infections (UTIs). Results show that Escherichia coli is the most common pathogen in UTIs, while a diverse range of microbes, including various fungi and gram-positive and gram-negative bacteria, were identified in both groups. The research emphasizes the need for targeted studies to understand the urinary microbiome's role and suggests antibiotic stewardship based on antimicrobial susceptibility testing.



























![infections-of-the-urinary-tract-220909145507-332a77e1 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/infections-of-the-urinary-tract-220909145507-332a77e1autosaved-240724052813-02564720-thumbnail.jpg?width=640&height=640&fit=bounds)







































