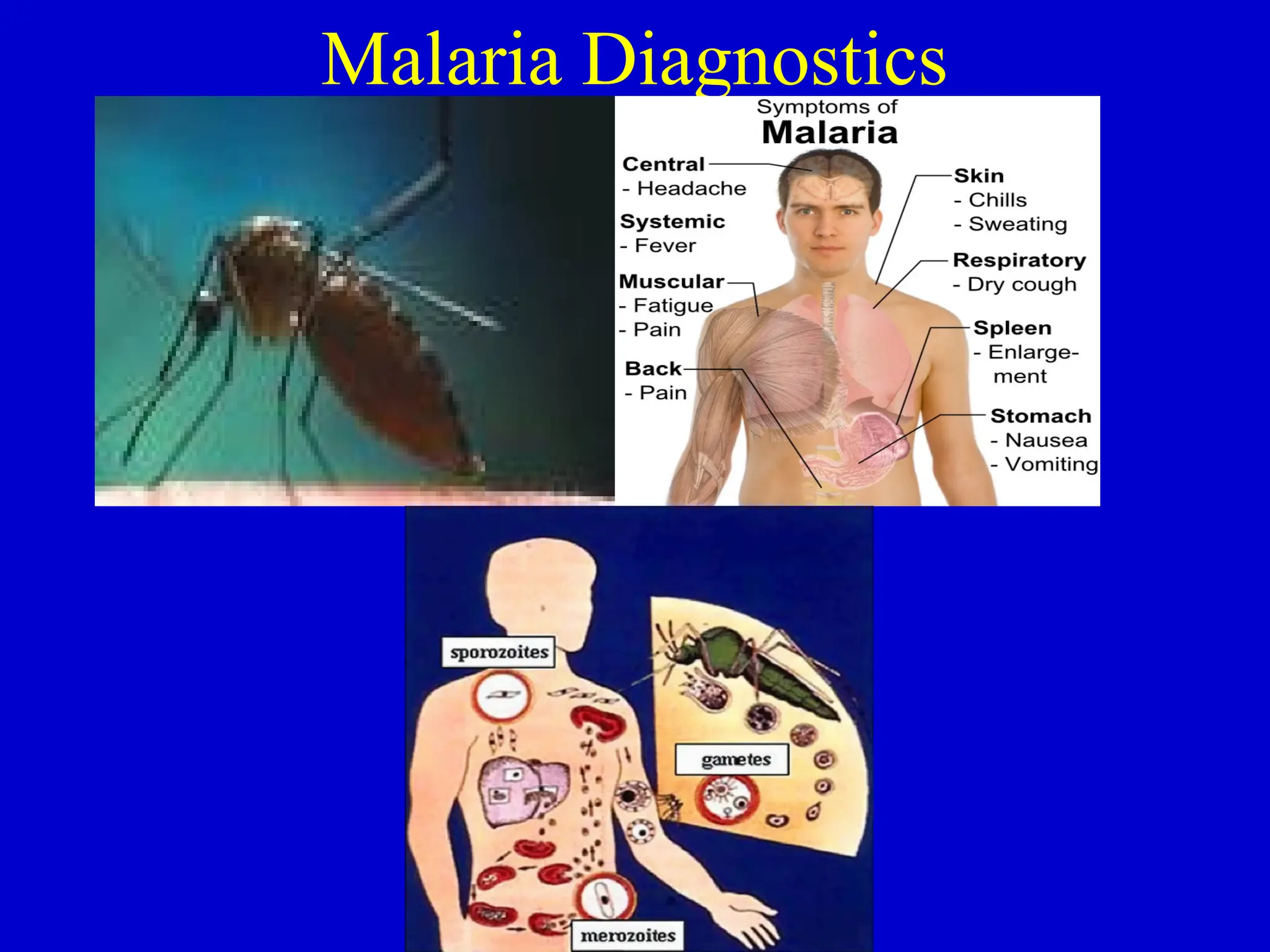
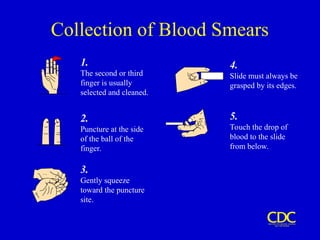
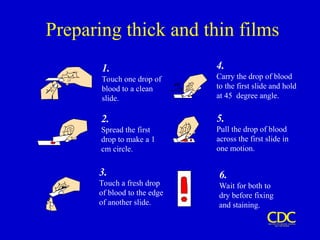
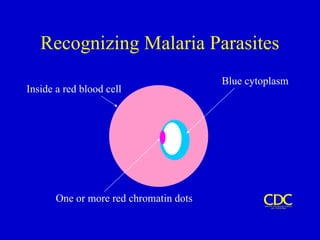
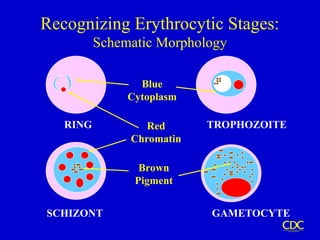
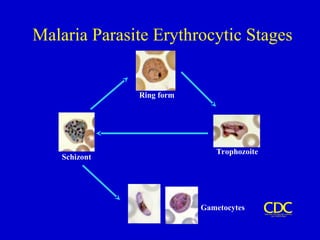
The document discusses malaria diagnostics, detailing various clinical and laboratory methods for diagnosing malaria, including blood smears, microscopy techniques, and antigen detection. It emphasizes the importance of accurate parasite identification and quantification, as well as the limitations and requirements of each diagnostic method. Additionally, it covers the interpretation of results and the significance of different species of Plasmodium in malaria diagnosis.



































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
