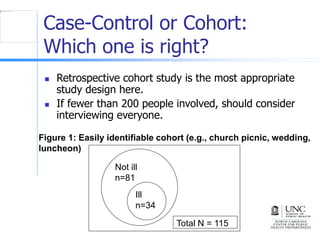
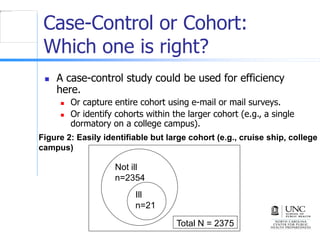
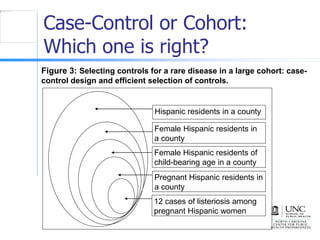
This document describes cohort and case-control study designs. Cohort studies follow groups over time to compare disease occurrence between exposed and unexposed groups. Case-control studies identify people with and without a disease and compare past exposures. Cohort studies are best when the entire population is identifiable, while case-control studies are more efficient when the population is large or undefined. The document provides examples of outbreak investigations that effectively used each design.















































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)

















