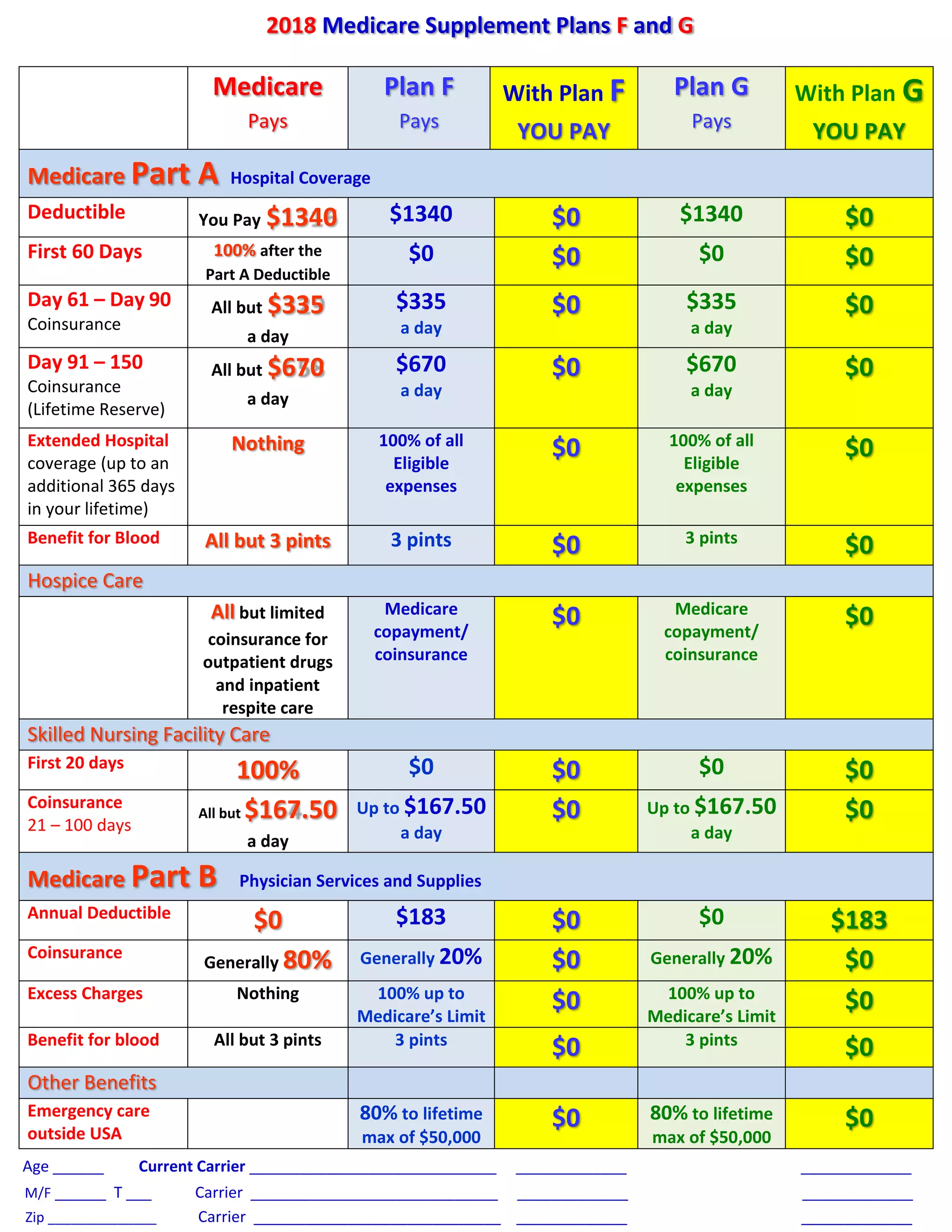
This document compares Medicare Supplement Plans F and G. Plan F pays all Medicare deductibles and coinsurance, so the individual pays $0 out of pocket. Plan G also covers Medicare deductibles but has a $183 annual deductible for medical services, so the individual pays that amount out of pocket plus any Medicare coinsurance. Both plans cover extended hospital stays, blood transfusions, hospice care, and skilled nursing facility care with no out of pocket costs. Plan F provides the most comprehensive coverage with $0 out of pocket costs.