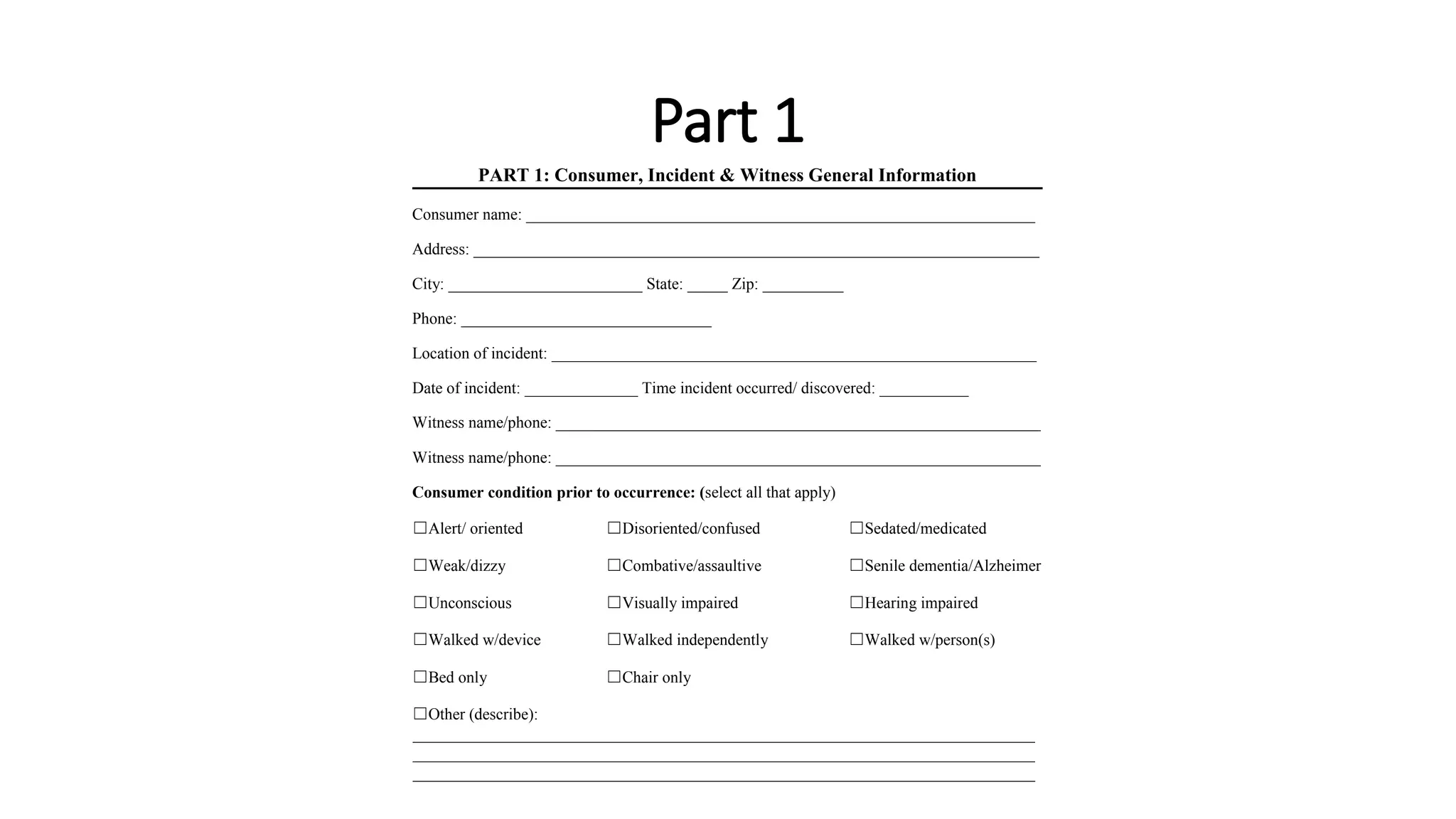
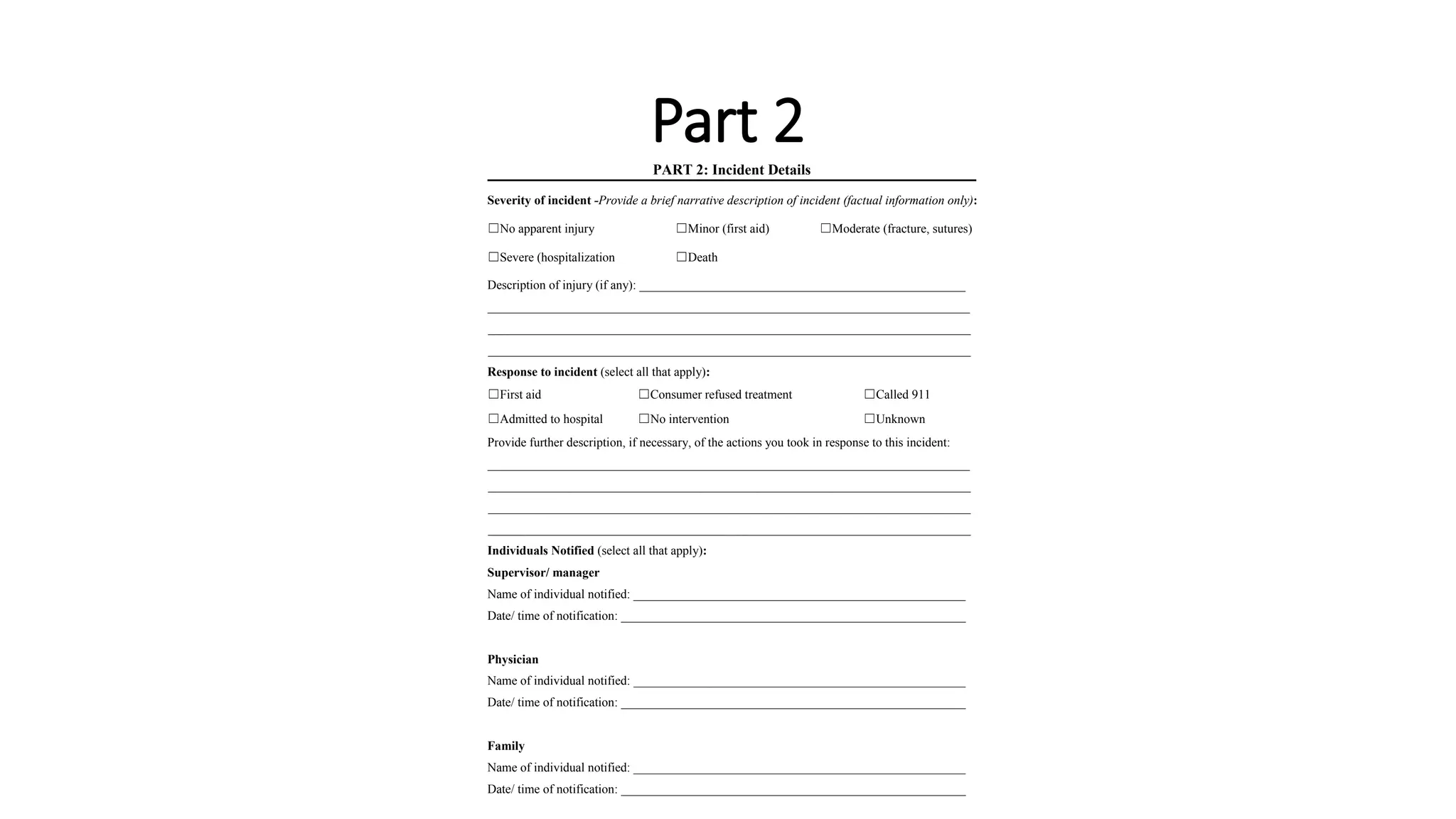
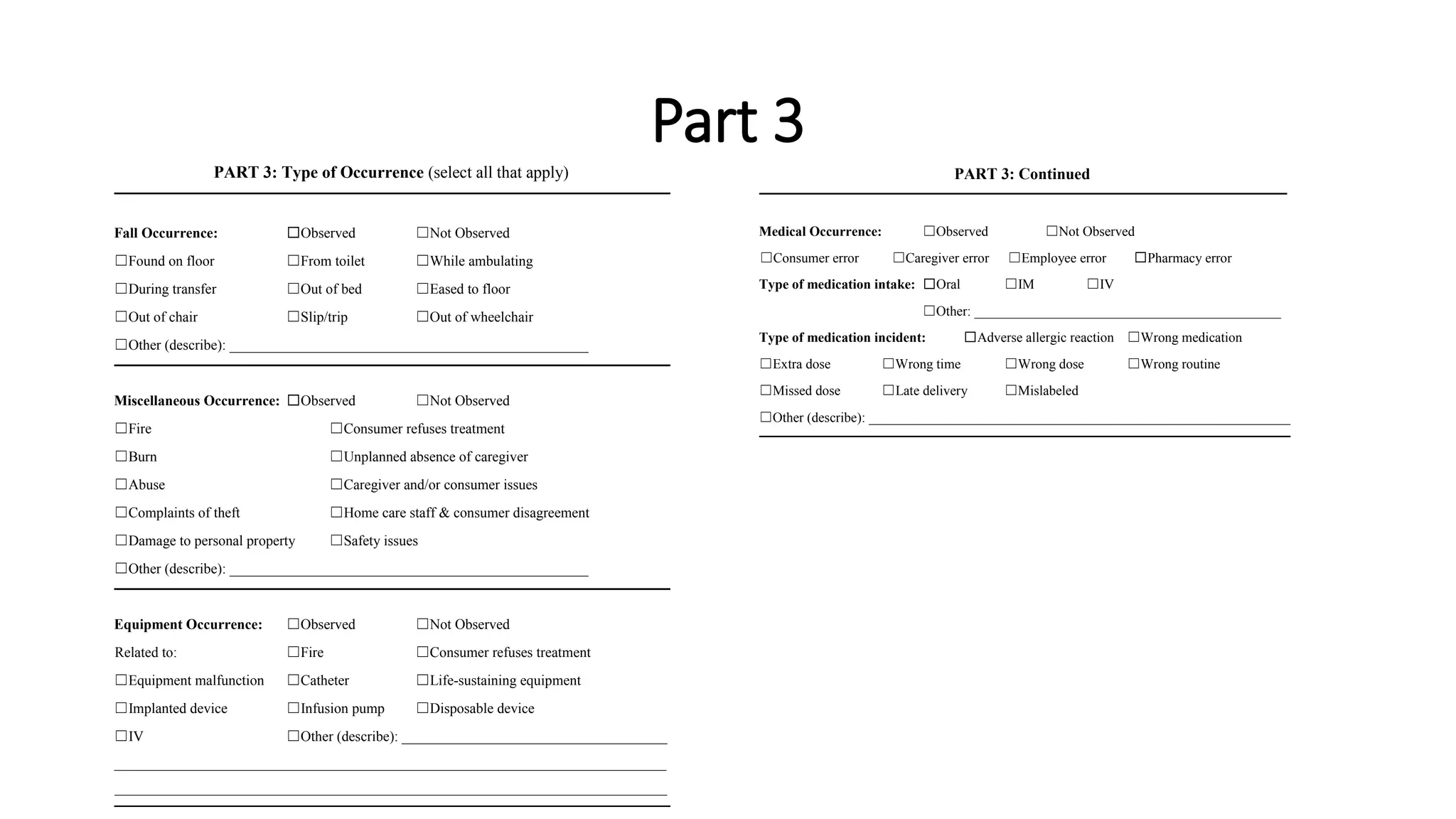
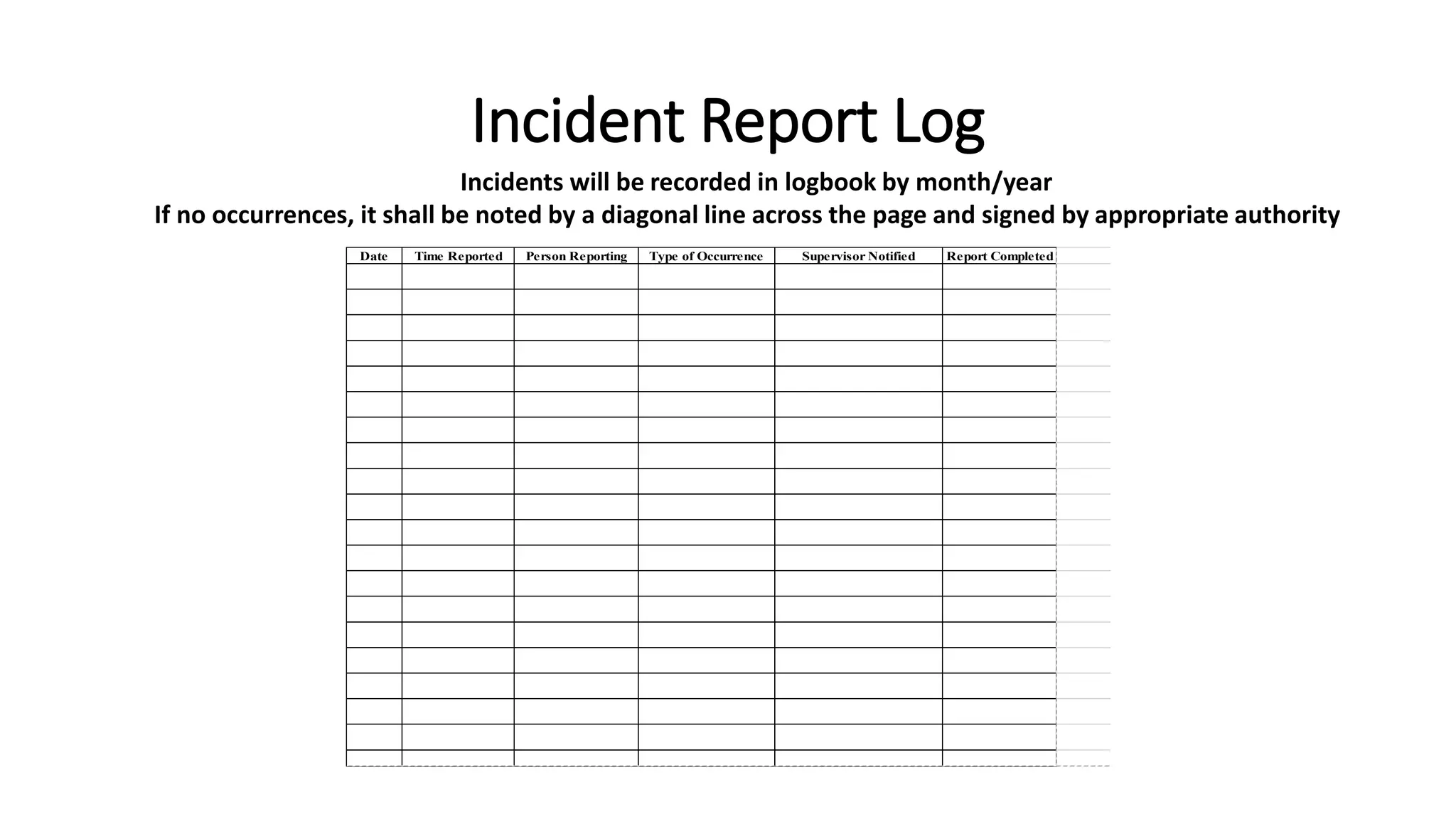
The document provides instructions for reporting incidents at a healthcare facility. It states that all incidents should be reported within 24 hours, and the employee's direct supervisor and any additional appropriate parties should be notified. The incident report has four parts: general information about the consumer and incident, details of the incident, type of occurrence, and a signature. It provides forms to fill out for each part, to collect information like consumer details, description of incident and injury, response taken, and parties notified.