

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Atrophic rhinitis.pptx
Similar to Atrophic rhinitis.pptx (20)
More from Sayan Banerjee
More from Sayan Banerjee (20)
Recently uploaded
Recently uploaded (20)
Atrophic rhinitis.pptx
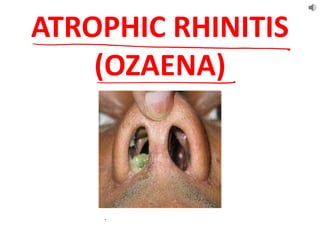
- 2. • DEFINITION: It is a chronic inflammation of the nasal mucosa resulting in atrophy , squamous metaplasia and crust formation due to periarterial fibrosis and end arteritis. • Key-points: – Atrophy of the nasal mucosa and turbinate. – Scanty viscid secretion – Loss of ciliated columnar epithelium – Crust formation
- 3. • TYPE: – Primary – Secondary: infection or surgery • Long-standing purulent sinusitis. • Iatrogenic: Radical turbinectomy, maxillectomy, post-radiotherapy. • Tuberculosis, Syphilis, Leprosy, Rhinoscleroma. • Deviated nasal septum (atrophy in wider nasal cavity). • FORM: – Rhinitis sicca : mild form – Severe form : ozaena • Turbinante atrophy • Squamous metaplasia • Degeneration of goblet cells • Secondary growth of saprophytes
- 4. Periarteritis + endarteritis of nasal mucosa Decreased blood supply Mucous glands decrease in number and size along with atrophy of the epithelium Metaplasia of the ciliated columnar epithelium to squamous epithelium Loss of cilia and decreased secretions Stagnation and stasis of viscid secretions Growth of viscid organisms PATHOPHYSIOLOGY:
- 5. ETIOLOGY PRIMARY : Not known
- 6. ETIOLOGY PRIMARY : Not known 1. Developmental: – Congenitally spacious nasal cavity – Poor pneumatization of maxillary antrum 2. Heredity: 30% cases autosomal inheritance; 67% = Dominant, 33% = Recessive. 3. Endocrinal: estrogen progesterone imbalance, common in female after puberty; Symptoms aggravated due to estrogen deficiency. 4. Race: white & yellow races >>> negroes 5. Malnutrition: chronic iron deficiency anemia, vitamin A & D deficiency 6. Chronic inflammation 7. Nasal and sinus suppuration: Klebsiella ozaenae (Perez & Abel bacillus), Coccobacillus foetides ozaena, Bacillus mucosus, Diphtheroids, Haemophilus influenzae, Proteus vulgaris, E. coli, Staphylocococci & Streptococci. 8. More common: Blood group O and B 9. Immunological factor: Altered cellular immunity and loss of tolerance of nasal tissue may trigger destructive autoimmune process on nasal mucosa. 10. Reflex sympathetic dystrophy syndrome (RSDS) causes vasodilatation & hyperaemic decalcification of turbinates followed by vasoconstriction. 11. Surfactant deficiency in nasal secretion: ciliary dysfunction + stasis of nasal secretions.
- 7. CLINICAL FEATURES • Age : Onset after puberty, 14-16 years • Sex: more in females • Race: Rare in negroes
- 8. SYMPTOMS • Nasal obstruction • Crusting • Anosmia • Headache • Epistaxis • Foetor SIGNS • Crust • Greenish discolouration • Roomy nose • Atrophied turbinates • Choana/ nasopharynx visible • Pus in the middle meatus • Posterior rhinoscopy MERCIFUL ANOSMIA
- 9. Causes of Anosmia • Loss of olfactory neural elements • Thick secretion & crusts over olfactory area • Degeneration of secretory glands → scanty mucous for dissolving odoriferous materials Causes of nasal obstruction • Blunting of sensory nerve endings • Crust formation • Lack of eddy current formation in roomy cavity
- 11. INVESTIGATIONS 1. Radiology: X ray PNS, CT scan of the PNS 2. Hematology: ESR, Sugar, Estrogen, Progesterone, Serology; Serum iron, vitamin-A/ D & protein levels- malnutrition 3. Pathology: Nasal swab- smear or HPE of nasal mucosa. 4. Saccharine test: ed nasal muco-ciliary clearance time. 5. Culture & sensitivity of nasal discharge.
- 13. There is a metaplasia of columnar or ciliated epithelium to squamous epithelium with decrease in the number of compound alveolar glands. Histopathologically, there are 2 types of atrophic rhinitis: Type I: Characterized by endarteritis and periarteritis, which may be as a result of chronic infection. These patients may benefit by vasodilator effect of estrogen therapy. Type II: Characterized by vasodilation of capillaries which may become worse by estrogen therapy. HISTOPATHOLOGY
- 14. D/D 1. Syphilis 2. Lupus 3. Leprosy 4. Tuberculosis 5. Rhinoscleroma 6. Sinusitis D/D for ozaena D/D for dry nose Atrophic rhinitis Atrophic rhinitis Purulent sinusitis Rhinitis sicca Nasal foreign body Radiotherapy Rhinitis caseosa Sjogren’s syndrome Malignancy
- 15. SPECIFIC INVESTIGATIONS TO RULE OUT OTHER D/Ds: 1. Chest X-ray: T.B., bronchiectasis, lung abscess 2. Serology for syphilis: V.D.R.L., T.P.H.A., T.P.I. 3. Sputum for AFB, Mantoux test: T.B. 4. Nasal smear study: Leprosy 5. Complement fixation test & biopsy: Rhinoscleroma
- 16. COMPLICATION • Nasal myiasis • Sinusitis
- 17. TREATMENT
- 18. ACTION OF PLACENTAL EXTRACT Progesterone leads to hyperplasia of nasal mucosa & glandular secretion Estrogen leads to vasodilatation Biogenic stimulator of metabolic & regenerative process Intra- placental serum boosts up immunity Mechanical narrowing of nasal passage
- 19. SURGICAL TREATMENT • Aim: – Decrease size of nasal cavity – Decrease air entry – Increase lubrication 1. Narrowing of nasal cavity: a) At lateral wall: i. Dermofat graft ii. Bone cartilage graft iii. Synthetic teflon paste or acrylic mould b) At floor: placental graft submucosally c) Young’s and modified young’s operation 2. Transplantation of parotid duct
- 20. TYPES OF SURGERY NASAL CLOSURE Young Modified Young VOLUME REDUCTION Lautenslager Wilson Sublabial implants Vestibuloplasty DENERVATION Cervical sympathectomy Stellate ganglion block Sphenopalatine ganglion block SALIVARY IRRIGATION Parotid duct implantation
- 21. AIM OF SURGERY
- 23. ADVANTAGES OF MODIFIED YOUNG’S SURGERY