❤️Chandigarh Escort Service☎️9815457724☎️ Call Girl service in Chandigarh☎️ C...
Smith-Lemli-Opitz Syndrome3
1. J. ment. Defic. Res. (1974) 18, 51 51
THREE SISTERS WITH THE SMITH-LEMLI-OPITZ
SYNDROME
SARAH BUNDEY
MRC Clinical Genetics Unit, Institute of Child Health, London
and
H. G. SMYTH
Clinical Director, Princess Marina Hospital, Norihants
INTRODUCTION
The Smith-Lemli-Opitz syndrome was first described in 1964, and since then a
total of forty-eight cases has been reported: twenty-nine males and nineteen females.
The syndrome was reviewed by Ghakanovskis and Sutherland (1971); further cases
have been reported by Lowry, Miller and Mclean (1968), Gotlier and Rice (1971),
Robinson, Perry, Barlee and Mellar (1971), Nevo, Benderly, Levy and Katznelson
(1972) and Garcia, McGarry, Voirol, Duncan (1973). We do not think the adult
reported by Fried and Fraser in 1972 had the syndrome, as he was not dwarfed and
did not have the characteristic facies. It is thought that the homozygous state of a pair
of autosomal recessive genes is the most likely aetiology (Opitz, Zellweger, Shannon
and Ptacek, 1969; Smith, 1970) although a hitherto undetected chromosome
abnormality has been suggested, in view of two families with affected cousins, and the
variety of malformations reported in association with the syndrome (Dallaire, 1969).
A family with three affected sisters is reported here to provide further evidence
for autosomal recessive inheritance. The children came to notice simultaneously, on
their admission to the Princess Marina Hospital.
Family Findings
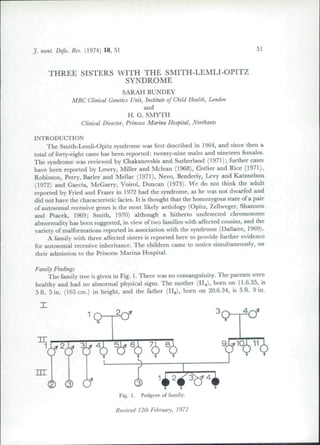
The family tree is given in Fig. I. There was no consanguinity. The parents were
healthy and had no abnormal physical signs. The mother (H^), born on 11.6.35, is
5 ft. 5 in. (165 cm.) in height, and the father (H9), born on 20.6.34, is 5 ft. 9 in.
Fig. 1. Pedgree of family.
Received 12th February, 1972
2. 52 SMITH-LEMLI-OPITZ SYNDROME
(175 cm.). Their chromosomes and dcrmatoglyphic fmdings were normal. They
have three mentally retarded and dwarfed daughters and one healthy son, a twin of
the second daughter. He had no abnormal physical signs, and measured 4 ft. 3 in. at
six years of age. His chromosomes and dcrmatoglyphic features were normal.
Case I (IIIi), born 9.4.62
She was born at forly-lwo weeks' gestation with a birth weight or4| Ib (2 kjj.). She had a
dislocated hip on the left which resolved spontaneou.sly. She was a difficult feeder and had to
be tube frd for five weeks. At two months she began to have momentary episodes when her
body would go stifT, her eyes would stare, and her right hand would jork. She had her first
grand mal attack at one year, and continues to have both grand mal and petit mal attacks.
She is on anticonvulsants. Her milestones were retarded; she sat at one year and stood with
support soon after. She did not become toilet traine-d, and did iiol learn to speak, and walked
with encouragement only at ten years. She was at liorne until tlie age of eight, when she was
taken into permanent care together with her two ailctted sisters. Physical examination in 1971
revealed a delightful, small, and severely retarded child. She was below the third percentile
for height and weight and her head circumference was that oi a fivc-month-oldgirl. Intelligence
testing on the Griffiths scale had shown her to be at an eighth-month level at eight yeai"s, other-
wise neurniogical examination was normal. Some of licr physical features are shown in Figs.
2-5 and described in Table. 1. Her head was long and narrow and sht; liad low-set unfolded
cars with preauricular sinuses. She had ptosis, cpicanihic folds and a broad base to her nose.
She had a cleft uvula, small mandible, long hypotonic fingers wilh proximally set thumbs, a
sacral dimple and feet deformities. She also had a precordial systolic murmur which was
associated with cardiomegaly on chest X-ray but with a normal ele( trocardiograni.
Palmar dermatoglyphics (sec Table 2 and Fig. 9) showed a large atd angle and a loop in the
fourth inierdigital area on the left. The karyotype was normal (46, XX). Electroencephalo-
graphy, performed on several occasions, showed abnormal results. In 1964 the record showed
severe generalised abnormality with frequent complex and unusual discharges, more obvious
Fig. 2. Case I at the agt; ()1 eighteen months.
Note the broad-base nose epicanthic folds,
unfolded ears and small jaw.
Fig. 3. Case i ai ilir age nl ciglitern inontlis.
Note the low-set unfolded car with a pre-
auricular sinus, the upturned nares and the
smalt lower jaw.
3. SARAH BUNDEY and H. G. SMYTH 53
Fig. 4. Cast 1 at nine and a half years. Note
the elfin-like featttres, broad base to the nose,
ptosis and unfolded ears.
Fig. 5. Case I at nine and a halfycars. Note
the low unfolded car and small mandible.
Fig. 6. Case 2 at six years, showing her epi-
canthic folds, broad-based nose, wide maxil-
lary ridges, and small mandible.
l-'ig. 7. Cast; 2 at six years.
over the posterior part of the head. In 1971 the report read "No alpha rhythm was detected.
Low voltage fast activity was widespread, persistent and mixed with random thela activity.
For considerable periods the record was relatively uneventful but the characteristic feature was
the occurrence of episodic bilateral post-central 4-7 c./sec. high voltage rhythms with a spiky
component ustially maximal on the right. 7 c./sec. activity was sometimes present posteriorly
at the same time as 4 c./sec. anteiiorly. Such episodes were often characterised by unusual
stillness."
4. 54 SMITH-LEMLI-OPITZ SYNDROME
Table 1
Symptoms and Signs of the Smith-Lemli-0pitz Syndrome and
Whether Present in the Three Sisters
Patient Case 1
Date of Birth 9.4.62
Symptons
Gestation Period (Weeks) 42
Birth Weight 4 lb 8 oz
Feeding Difficulties Yes
Epilepsy and Age at Onset -F(2/12)
Delayed Physical Growth -J-
Delayed Motor Development -f.
Signs
Date of Examination 14.12.71
Delightful Personality -|-
Able to Walk Alone
Intelligence level
Height in Inches 42
Head Circumference (Inches) 16.75
Long Narrow Head -|-
Low-set Ears -j..
Unfolded Ears --
Preauricular sinus -f-
Ptosis -|-
Epicanthic folds ...f-
Wide Bridge of Nose -f
Anteverted Nostrils 4-
Cleft Uvula +
Broad Maxillary Ridges -f-
Small Mandible -|-
Long Tapering Fingers -.|-
Low Set Thumh -(-
Simian Crease No
Syndactyly or Polydactyly No
Flexion of Hands, with Overriding
Index Finger -j-
Acrocyanosis of Hands -j-
Brisk Reflexes -|-
Hypotonia -|-
Hypertonia No
Ataxia No
Valgus Flexion Deformity of Elbow No
Wide-apart Nipples 4.
Heart Murmur 4-
Sacral Dimple -f
Abnorma! External Getiitalia No
Dislocated Hip L only
Vertical Talus -|-
Metatarsus Adductus 4-
Case 2
7.1.65
41
5 1b
Yes
+ (6/12)
14.12.71
Case 3
4.11.67
41
5 lb 3 oz
Yes
+ (3/12)
14.12.71
Yes Yes No
8/12 at 8 yrs 10/12 at 5 yrs 10/12 at 3 yrs
40.5 33
15.5
No
R only
No
No
No
No
No
No
No
No
No
No
No
No
No
15.0
R only
No
No
No
No
No
No
No
No
+
No
+
No
No
No
No
5. SARAH BUNDEY and H. G. SMYTH
Table 1 {continued)
55
Investigations
X-ray of Hands
X-ray of Chest
X-ray of Skull
EEG (see text)
Chromosomes
DermatogIyphics
ECG
Cataracts or retinal pigmentation
Renal abnormality
Delayed
bone age
Large heart
Normal
Abnormal
Normal
Not done
Normal
No
Normal
Normal
Abnormal
Normal
(See text)
Normal
No
(IVP not performed)
Not done
Normal
Normal
Normal
Normal
Normal
No
Fig. 8. The three sisters aged nine
and a half, six and four years. Note
ihcir small size, their widely separated
nipples, knobbly knees, and metatarsus
adductus in Case 1 on the right. Case
2 in the middle was the only girl who
could stand unsupported when the
photograph was taken.
She was the first of twins boin at forty-one weeks' gestation. She weighed 5 lb; her twm
brother 7i lb (3 4 kg.). She was a poor feeder in infancy. Grand mal convulsions began at six
months! and at nine months she developed spells oi becoming blank and pale with some
gasping She now has infrequent fits and is on anti-convulsants. Her milestones of developmen
were delayed, but not so much as in her older sister. She walked alone at three years, did not
become toilet trained nor learnt to speak. She was taken into permanent care at five years and
was round to be a severely retarded dwarfed girl with the same physical features as her sister^
Some of these are shown in Figs. 6 and 7 and are listed in Table 1. Exammatton m 1971 revealed
a retarded girl, below the thud percentile for height and weight and with a head circum-
ference helow 3 SD for her age and sex. Her intelligence on the Griffiths scale had been shown
7. SARAH BUNDEY and H. G. SMYTH 57
Fig. 9 (contd). 4, Case 1; 5, Case 2; 6, Case 3.
8. 58 SMITH-LEMLI-OPITZ SYNDROME
8 o
o
CO CO
[£;.£
o o
o 5
coco
— — o
2 =^o o
CO CO
o o
o o
CO CO
o o
o o
CO en
Jed
'a.
.a
.D.
'a
o.
,1
O
O
O 88 o o
o o
in m
2 oo oip in in 1/1
o'o'
"3
-4 oi ai Jo:
V
-a
ffi
.3
X
9. SARAH BUNDEY and H. G. SMYTH 59
lo be at a ten-month level at five years. She, like her sister, had a long narrow head, with low-
set ears, ptosis, epicanthic folds, a broad-based nose with anteverted nostrils and a small
mandible. She had long fingers with low set thumbs and had valgus deformities of her elbows.
Her nipples were widely spaced. She had brisk tendon jerks but no abnormal signs in the
nervous system, other than the retardation.
Palmar dermatoglyphics (Table 2 and Fig. 9) showed eight out often fingers had whorls, a
total ridge count of 175, and a loop in both fourth interdlgital areas. Karyotyping showed a
normal 46, XX constitution. Electroencephalography in 1971 was reported: "Beta activity
of varying amplitude was widespread, persistent and mixed with random intermediate slow
elements. Post-central activity within the alpha range was present but usually obscured by
other rhythms. With the eyes open brief post-central symmetrical runs of medium-high
amplitude rhythmic activity at 6-8 c./sec. were seen, and eye closure resulted in more wide-
spread higher amplitude and slower paroxsyms which might persist for the whole period of eye
closure. High voltage posterior rhythmic activity at 4 c./sec. was occasionally present on its
own. Comment: This is a severely abnormal record with irequent symmetrical paroxysmal
discharges. These are of unusual type and may be interpreted as indicating both cortical and
subcortical lesions. They are similar to those seen in her older sister's record."
Case 3 (III4), born 4.11.67
She was bom at forty-one weeks' gestation, by Caesarian section performed for foot
presentation. She weighed 5 lb 3 oz (2.36 kg.) at birth, was a difficult feeder and initially
had to be fed three-hourly. At three months she had her first convulsion and at six months
developed minor blank spells, similar to those of her sisters. She continued to have both sorts of
attack and recently had a prolonged hemiplegia after a grand mal convulsion. Her milestones
have been severely delayed and she neither walks nor stands, says no words, and is not toilet
trained. Like her sisters she has a delightful affectionate personality.
Examination in I97I showed that she was well below the third percentile for height and
weight and her head circumference was below 3 SD for sex and age. Intelligence on the
Griffiths scale had showed her to be at a ten-month level at three years. She had similar physical
features to tbose of her sisters; see Fig. 8 and Table I. Her palmar dermatoglyphics (Table 2
and Fig. 9) showed five whorls, a total ridge count of 141, a maximum atd angle of 136, and
a loop in the fourth interdigltal areas. The karyotype was that of a normal 46, XX female.
The EF,G was normal apart from an occasional right posterior discharge.
Topological description and analysis of hand and foot prints of the family
(Table 2) was provided by Dr. Loesch who reports as follows: "It happens thai in
both affected and unaffected members of the family, some palmar and sole pattern
combinations are of a common type and some are rather rare. The patterns of the
afTeeted children do not differ considerably from those of their parents, except for the
presence of the hypotbenar distal H loop, present in two of tbe tbree affected children
but not in any normal members of the family."
DISCUSSION
In 1964, Smitb et al. produced tbe first description of tbis syndrome in tbree
unrelated boys, altbough it was likely tbat tbe deceased brotber of one of tbem had
also been affected. Since tben forty-five furtber cases bave been reported and a clear
picture of the syndrome is emerging. Clinical features are listed in Table 1. Tbe
main manifestations are mental retardation and dwarfism, and tbese, togetber
witb tbe characteristic facial appearance (ptosis, broad-based nose witb upturned
10. 60 SMITH-LEMLI-OPITZ SYNDROME
nares, low, unfolded ears with preaurieular sinuses and a stnall mandible) and the
abnormal gcnitalia in boys are ustially sufficient to make llie diagnosis. However, in
an infant wbo also has cardiac, genital and feet abnormalities the clinical picture
may be confused witb tbat of trisomy-18. Features present in tbe original patients
reported and not pre.sent in tbese three sistci's, were genital abnormalities (bypo-
spadias, a tetbered and incompletely formed scrotum and cryptorchidism) and pyloric
stenosis. A variety of other abnormalities bave been reported since, and pleiotropic
manifestation is a remarkable feature of tbi.s syndrome. Tbe furtber abnormalities
include cleft palate, polydactyly or syndactyly, anatomical renal abnormalities,
congenital beart disease of various sorts, congenital dislocation of the hips, cataracts
and retinal pigmentation. Neurological complications, otber than severe mental
retardation and variably altered musele tone, are rare. Fits have been reported in
five previous cases, in tbree instances being associated witb a dysrhytbmie electro-
encepbalogram. In seven other cases EEG abnormalities have been reported in tbe
absence of fits. The sisters reported here have epilepsy whicb is controlled btit two
of tbem bave very unusual EEG's suggesting multiple cerebral lesions. Malformations
of tbe central nervous system bave been inconsistent in those children wbo have come
to autopsy or who bave been studied in life. Three bad various structural abnormalities
of tbe brain and spinal cord, while four bad small but otberwise macroscopically
normal brains (Fine, Gwinn, and Young. 1968; Opitz ei al,, 1969; Cbakanovskis and
Sutberland, 1971; Robinson et al., 1971; Garcia et al., 1973).
Palmar dermatoglyphics in reported cases, bave sbown a tendency to an
increased number of wborls, a reduced number of ulnar loops, and a high total ridge
count. In tbe family we bave described, tbe latber, wbo is normal, has six wborls
on bis fingers and a loop in tbe fourth interdigital area on both sides. Often tbere are
abnormalities of the palmar creases too. In addition, tw'o of our patients have an
increased atd angle and all bave a loop in tbe fourth interdigital area. The H loop
is the one feature wbich is present in two affected subjects but no normal members
of tbe family.
Tbe varied manifestations and the inclusion ol" malformations known to be
polygenieally inherited (pyloric stenosis, congenital heart disease) suggest tbat a
group of genes might be aetiologically responsible. Howc'er, karyotypes on these
and other patients have been normal, and family data strongly suggest autosomal
recessive inheritance. For secondary cases, apart from two affected cousins reported
by Dallaire in 1969, have all been sibs; and tbere bave been two instances of con-
sanguinity {Dallaire, 1969; Nevo et al, 1972). Males and females are botb affected,
tbe slight male excess probably being due to an ascertainment bias, owing to the
genital abnormalities present in males (Opitz et al, 1969; Smith 1970). Tbe occur-
rence here of tbree affected sisters born to normal parents is fuiiher evidence for
autosomal recessive inheritance. It is likely that tbe recessive gene is relatively
common in view of the large nunilicr of cases recognised since 1964 and tbe report
of affected cousins by Daliairc. Tbe mechanism whereby the bomozygous state ofa
pair of genes produces such a variety of manifestations is not clear.
11. SARAH BUNDEY and H. G. SMYTH 6.1
SUMMARY
Tbree sisters born to normal parents have tbe Smitb-Lemli-Opitz syndrome
with epilepsy and electroencephalographic abnormalities. Their karyotypes were
normal. The family provides further support for autosomal recessive inheritance of
this syndrome.
ACKNOWLEDGEMENTS
We are grateful to Dr. I.oesch and Dr. David Hughes for analysing the dermato-
glyphics and for performing the chromosome studies, to Dr. Peter Payan for his
reports of the EEG's, and to the Department of Medical Illustration, Institute of
Child Health, The Hospital for Sick Children, for the photographs. We thank
Dr. B. W. Richards for his helpful comments on the family.
REFERENCES
CHAKANOVSKIS, J. E. and SUTHERLAND, G. R. (1971) The Smilh-Lemli-Opitz syndrome in a
profoundly retarded epileptic boy. J. ment. Defic. Res. 15. 153.
CoTLiEn, E. and RICE. P. (1971) Cataracts in the Smilh-Lemli-Opitz syndrome. Amer. J.
Ophthai 72, 955
DAt.L.iRE, L. (1969) Syndrome of retardation with urogenital and skeletal anomalies (Smith-
Lemli-Opitz syndrome). J. Aled. Genet. 6, 113.
FINE, R . N . , GWINN, J. L. and YOUNC, E. F. (1968) Smilh-Lemli-Opitz syndrome. Amer. J.
Dis. Child 115, 483.
FRIED, K . and FRASER, W . I. (1972) The Smith-Lemli-Opitz syndrome in an adull. J. ment.
Defic. Res. 16, 30.
GARCIA, C . A., MCGARRV, P. A., VOIROT., M . and DUNCAN, C . (1973) Neurological involve-
ment in the Smith-Lemli-Opitz syndrome. Develop. Med. CJnld Neiirol. 15, 4H.
LOWRY. R . B.. Mn.r.ER. J. R. and MACLEAN, J. R. (1968) Micrognathia, polydactyly and cleft
palate. J. Pediat. 72, 859.
NEVO, S., BENDERLY, A.. LEVY, J. and B.^T-MIRIAN KATZNEI.SUN, M . (1972) Smith-Lejnli-
Opitz syndrome in an inbred family. Amer. J. Dis. Child. 124, 431.
OPITZ,J. M., ZELLWEGER, H . , SHANNON, W . R . and PTACEK, L.J. (1969) The RSH syndrome.
In The Clinical Delineation of Birth Defects, Part II, pp. 43-52. Published The National
Foundation March of Dimes.
ROBINSON, C . D.. PERRY. L. W . , BARI.FE. A. and MELLA, G . W . (1971) Smith-Lemli-Opilz
syndrome witli cardiovascular abnormality. Pediatrics. 47, 844.
SMITH, D. W . (1970) Recognizable patterns of human malformation, p. 136. Published W. B.
Saunders.
, D. W., LEMLI. L. and OPITZ, J. M. (1964) A newly recognised syndrome of multiple
congenital abnormalities. J. Pediat. 64, 210.