Physiologic changes in pregnancy assighnment.pptx
•Download as PPTX, PDF•
0 likes•26 views

Physiologic changes in pregnancy, in obstetric practice

Recommended
Recommended
More Related Content
Similar to Physiologic changes in pregnancy assighnment.pptx
Similar to Physiologic changes in pregnancy assighnment.pptx (20)
More from Lando Elvis
More from Lando Elvis (20)
Recently uploaded
Recently uploaded (20)
Physiologic changes in pregnancy assighnment.pptx
- 2. Jens Martensson 2 . . OUTLINE Definition Normal changes -CV -Respiratory -Hematologic -Endocrine -Urinary -GI -Reproductive organs -Skin -Musculoskeletal Implications for pathological conditions. Pregnancy as a “stress test for life” Unveils problems that will appear later.
- 3. Jens Martensson . THE CHANGES THAT TAKE PLACE IN THE MATERNAL ORGAN SYSTEM IN RESPONSE TO PREGNANCY. TO ACCOMADATE THE PREGNANCY AND TO PREPARE THE WOMAN FOR LABOUR Definition 3
- 4. Jens Martensson 4 Metabolic and endocrine changes HORMONES OESTROGEN • Produced in corpus luteum • Produced by placenta after 12 weeks • Responsible for growth particularly of uterus and breasts • PROGESTERONE • Produced in corpus luteum and then the placenta • Relaxes smooth muscle • Inhibits uterine contractions until uterus is prepared for labour • Regulates storage of body fat
- 5. Jens Martensson HUMAN CHORIONIC GONADOTROPHIC • RELAXIN 5 HORMONES cont. • Secreted from trophoblast of the developing embryo • Maintains corpus luteum until placenta takes over • Used in tests to confirm pregnancy • HUMAN PLACENTAL LACTOGEN • Alters maternal metabolism • Diverts glucose to fetus • Mobilises free fatty acids from maternal stores • Released by corpus luteum then the Placenta • Softens pelvic ligaments • Reduces myometrial tone • Relaxin peaks in early and late pregnancy. Women with chronic joint instability may notice an increase in symptoms during these times.
- 6. Jens Martensson • NOTE • Edema is present in the hands. feet. face and eyelids. This is due in part to sodium and water retention. Additionally. hormones circulating by the placenta. ovaries, and adrenal cortex cause increased capillary permeability, which contributes to the edema many pregnant women experience. 6 Metabolic and endocrine changes cont... Endocrine (insulin) changes: -Pregnancy is diabetogenic due to placental hormones (Placental lactogen, HGH, cortisol, progesterone). -Insulin requirement increases during pregnancy. -Insulin requirement falls abruptly after delivery. • Anti-insulin environment is aided by: • placental lactogen • Like growth hormone • Increases lipolysis and FFA • Increases tissue resistance to insulin • Increased unbound cortisol
- 7. Jens Martensson 7 Metabolic and endocrine changes cont... • BMR increases by 20-25 % during pregnancy • Recommended weight gain – 25-35 lb • Overweight – 15-25 lb • Underweight – 25-35 lb • Need for increased iron, calcium, fat, and protein • Caloric requirements increases by ~ 300 calories/day • Increase in Protein and fluid requirements . METABOLISM
- 8. Jens Martensson 8 Metabolic and endocrine changes cont... • Estrogen stimulates Increase in TBG • Total T3 and T4 are increased • However the active hormones remains unchanged • hCG stimulates thyroid • TSH is reduced • Iodine deficient state • Due to Increased renal clearance • To rule out pathologic changes • Early in pregnancy TSH can be used • Later free T4 is needed LIVER • Liver morphology unchanged • Lab Tests similar to liver disease • Alkaline phosphatase doubles • AST, ALT, GGT and bilirubin are slightly lower • Decreased plasma albumin • GALBLADER • Impaired contraction. . High residual volumes • Promotion of stasis • Stasis associated with increased cholesterol saturation of pregnancy, supports predisposition of stones • Intrahepatic cholestasis THYROID
- 9. Jens Martensson CARDIOVASCULAR CHANGES 9 Growth Shows Sales To meet increased metabolic demand. -Increased blood volume(50%) / RBC mass -Reversible cardiac hypertrophy (30%?) -Decreased Hct and viscosity -increase in SV(25 – 30%) -increase in cardiac output -increase in HR at given work load -increase in blood volume (mostly during latter half of pregnancy) -Uterus may compress large blood vessels reducing venous return
- 10. Jens Martensson Cardiovascular Changes 10 DECREASE -Hematocrit -Blood pressure -Blood supply to uterus -Cardiac reserve -Vascular resistance Heart shifts up and to the left Hemoglobin stays the same (12- 16 g/dL) initially May drop down to 10 g/dL and still be normal physiologic anemia. Normal pregnancy Hgb is 10- 14 g/dL later in pregnancy Decreased Hct (38-47%) Normal pregnancy Hct is 32-42 later in pregnancy Pulse rate may increase 10-15 beats. Weight of uterus can cause supine hypotensive syndrome. INCREASE -Blood volume -Cardiac (heart) output -Stroke volume -End diastolic volume -Resting pulse -% of blood plasma
- 11. Jens Martensson Supine hypotension related to Venal cava syndrome 11 This leads to dizziness, air hunger, nausea 2.5 3.5
- 12. Jens Martensson Total body water 12 -Increases 6-8 L -Increases by 40 % -Normal body water 2/3 intracellular 1/3 extracellular ¾ interstitial ¼ intravasular -2/3 increase is extravascular
- 13. Physiologic anemia of pregnancy Physiologic intravascular change Plasma volume increases 50-70 % Beginning by the 6th wk RBC mass increases 20-35 % Beginning by the 12th wk Disproportionate increase in plasma volume over RBC volume---- Hemodilution Despite erythrocyte production there is a physiologic fall in the hemoglobin and hematocrit readings
- 14. Jens Martensson Cont… • With erythropoiesis of pregnancy, iron requirements increase. • Because large amounts of iron may not be available from body stores and may not be in the diet • Supplementation is recommended to prevent iron deficiency anemia • At term, Hemoglobin less than 10.0 is usually due to iron deficiency anemia rather than the hemodilution of pregnancy Normal Iron Requirements • Total body iron content average in normal adult females is 2gm • Iron requirement for normal pregnancy is 1 gm • 200 mg is excreted • 300 mg is transferred to fetus • 500 mg is need for mom • Total volume of RBC inc is 450 ml • 1 ml of RBCs contains 1.1 mg of iron • 450 ml X 1.1 mg/ml = 500 mg • Daily average is 6-7 mg/day • Small intervals between pregnancies are most concerning Iron deficiency anemia
- 15. Jens Martensson 15 RESPIRATORY SYSTEM CHANGES • Mechanical • diaphragm • Consumption • Increase in needed oxygen • Stimulation • Progesterone stimulation Respiratory Changes Respiratory Changes Respiratory capacity Respiratory capacity increases increases Shortness of breath Shortness of breath Pulmonary reserve Pulmonary reserve decreases decreases Increased risk of Increased risk of muscle soreness muscle soreness Tendency to Tendency to hyperventilate hyperventilate RESULT RESULT adjust the intensity level and duration of exercise adjust the intensity level and duration of exercise
- 16. Jens Martensson • increase respiratory rate • increased oxygen consumption • common are nasal stuffiness, nosebleeds due to Increased vascular swelling to nose 16 RESPIRATORY SYSTEM CHANGES cont… • Consumption • O2 consumption Increases 15-20 % • 50 % of this increase is required by the uterus • Despite increase in oxygen requirements, with the increase in Cardiac Output and increase in alveolar ventilation oxygen consumption exceeds the requirements. • Therefore, arteriovenous oxygen difference falls and arterial PCO2 falls.
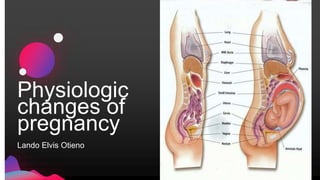
- 17. Jens Martensson • Displacement of the stomach and intestines • Appendix can be displaced to reach the right flank • Gastric emptying and intestinal transit times are delayed secondary to hormonal and mechanical factors • Pyrosis is common due to the reflux of secretions • Vascular swelling of the gums • Hemorrhoids due to elevated pressure in veins 17 PHYSIOLOGIC CHANGES IN GASTROINTESTINAL • Digestive system slow due to progesterone • Nausea and vomiting(hyperemesis) • Ptyalism: increase salivation • Heartburn • Hemorrhoids • Prolonged gallbladder emptying time may lead to gall stones • Bile salt buildup may lead to itching.
- 18. Jens Martensson • Uterus – • Enlarges : esp fundal area thickens, then thins later in preg • Umbilicus by 20 weeks • Xyphoid by 36 weeks fundus, Braxton-Hicks irregular contractions after 4 months • Cervix – mucous plug, Goodell’s sign, Chadwick’s sign. • Length remains the same • Increase in width • Softening after third month due to oestrogen • Increased vascularity • Increased cervical mucosa • Increased glandular function 18 Physiologic changes in pregnancy - Reproductive system • GENITAL TRACT • Increased vascularity and hyperemia • Vagina • Perineum • Vulva • Increased secretions • Characteristic violet color of the vagina • Chadwick’s sign • Increased length to the vaginal wall • Hypertrophy of the papillae of the vaginal mucosa
- 19. Jens Martensson 19 Relative Uterus Size During Pregnancy • uterus grows to 30x23x20 at term weight increases to 900gms • hypertrophy.. Oestrogen causes cells to increase until 20 weeks gestation • Hyperplasia:- number of cells increase under the influence of oestrogen • After 20 weeks of gestation: Uterine muscle tissue stretches to allow fetus to grow, and Progesterone relaxes the smooth muscles enabling it to stretch
- 20. Jens Martensson • By 2ND TRIMESTER • Development of the upper and lower uterine segment • Upper segment, thicker containing oblique muscles • Lower segment formed from the isthmus contains circular and longitudinal muscles • Uterus is pear shaped again • Braxton Hicks contractions • BY 3RD TRIMESTER • Lower segment formed from isthmus and contains longitudinal fibres .Upper segment thick and contains oblique muscle fibres • By 36 weeks lower segment measures 8-10cms • Engagement • By 38 weeks the cervix is taken up into the 20 Changes in the shape of the uterus • Isthmus elongates during the 1st 10 weeks like a stalk • From 7mm to 2.5cms at 10 weeks • Later becomes the lower segment with the globular uterus sitting on top • By 12 weeks • Uterus is upright and leans slightly to the right • No longer a pelvic organ • Uterus may be palpable above the pubic bone • Fetus now occupies most of the uterine cavity • Placenta now developed
- 21. Jens Martensson 21 BLOOD SUPPLY TO UTERUS CHANGES • Blood supply pre pregnancy = 10mls/min • At 40weeks 800 – 900mls/min • 20% of cardiac output goes to uterus
- 22. Jens Martensson • PHYSIOLOGIC CHANGES • Urinary tract changes result form the inc blood volume and glom filtration rate and inc fundal size puts pressure on internal organs • More susceptible to infection dt dec blood flow and traumaGFR raises by 50% • Increased renal clearance leads to lowered BUN and nonprotein nitrogen values. • Renal plasma blood flow increases 50% • Glomerular Filtration Rate increases • Bicarbonate increased excretion • Creatinine increased excretion • Renal pelves and ureters dilate • Smooth muscle of bladder relaxes/stasis • Sugar may spill at 160/protein PIH 22 RENAL SYSTEM • Dilation of the renal vessels • Due the effects of progesterone • Increased renal blood flow • Gfr increases by 60% in early pregnancy • Size of pores increased • URINARY CHANGES • Kidneys grow and filter more blood as the blood volume increases • Become more susceptible to bladder and kidney infections • Bladder becomes compressed causing frequent urination and
- 23. Jens Martensson Pigmentation: It is due to suprarenal changes, it usually begins to appear after the 4th month. The pigmentation may appear anywhere but the commonest sites are: 1. Linea nigra: which is a line of pigmentation between the umbilicus and the symphysis pubis. 2. Increased pigmentation of the nipple as primary areola and appearance of the secondary areola. • MOST OF THESE RESOLVE AFTER PREGNANCY 23 Integumentary system physiologic changes Due to overstretching of the skin, the elastic fiber may rupture together with small blood vessels and so red streaks appear; known as striae gravidarum. They are usually more marked below the umbilicus, on the breasts and may appear on the buttocks and thighs. In some women they are not marked or even don't appear during pregnancy. After labour, the red striae become pale silvery white due to fibrosis and are known as (striae albicantes).
- 24. Jens Martensson • Stria gravidarum 24 Integumentary system physiologic changes…cont • Linea nigra
- 25. Jens Martensson 25 Integumentary system physiologic changes…cont 3. Cloasma gravidarum/ Melasma or mask face of pregnancy which is butterfly pigmentation of the forehead, nose, upper lip and the adjoining parts of the checks. This pigmentation may persist but the cloasma gravidarum usually disappears. Falling of hairs and brittleness of nails may occur during pregnancy.
- 26. Jens Martensson 26 Breast Changes -Early in pregnancy, tenderness and tightness is common -After 8 weeks, breasts grow and blood vessels often are visible -Nipples become larger and darker -A thick yellowish fluid can be expressed from the nipple
- 27. Jens Martensson Postural changes: During pregnancy, postural changes occur to accommodate for abdominal growth. a. These changes include forward head, rounded shoulders, increased lumbar lordosis, hyperextended knees, and pronated feet. b. The center of gravity changes, resulting in changes in balance. c. Muscular changes are also typical. often noted alterations include shortened hip flexors, lower back musculature, and pectorals. Abdominal muscles, neck, and upper back muscle groups elongate. This 27 Musculoskeletal system changes • Diastasis recti: separation of rectus abdominous : Abdominal muscles are stretched to the point of their elastic limit by the end of pregnancy. • Hormonal influence on the ligaments is profound producing systemic decrease in ligamentous tensile strength and an increase in mobility of structures supported by ligaments and may predispose the patient to joint injury especially in the weight-bearing joints of the back, pelvis and lower extremities. The pelvic floor muscles must withstand the weight of the uterus, the floor drops as much as 2.5 cm. Bones and joints:There is tendency to decalcification of bones, sublaxation of joints due to softening of ligaments by relaxin hormone. It is more marked in sacroiliac joint
- 28. Jens Martensson • Brain adaptations • Not really understood (progesterone metabolites on GABA pathways?), but the neuroendocrine response to stress is reduced in pregnancy. • Pituitary increases in size during pregnancy • Due to increased prolactin and ACTH secretion from AP • And increased oxytocin production from PP (where it is stored until progesterone levels drop) 28 Neurological and sensory Changes • Decreased intraoccular pressure • Corneal thickening • Altered sense of smell • Decreased attention span • Problems with memory • Altered CNS physiology leading to mood disturbance.
- 29. Jens Martensson SUMMARY 29 In summary, pregnancy alters the body from head to toe. The effects of these changes vary as the pregnancy progresses through the trimesters. In the first trimester, the baby begins to grow and the mother experiences increased urination, changes in skin and hair, and a thickening waistline. Changes in the cardiovascular system and metabolism can cause nausea and fatigue. In the second trimester, the baby's weight increases from an ounce to more than a pound. The pregnant soldier’s energy level improves, but she may experience heartburn, leg cramps, and her pelvis may relax causing discomfort to her sacro-iliac joint. During the third trimester, the baby has more rapid growth and weight gain. The pregnant soldier may have backaches, swelling of the hands, legs, and feet, and may feel warmer. She may experience breathlessness and more frequent urination as additional weight is placed on the bladder. Most changes that occur will be normal and will go away after delivery.
- 30. .
- 31. Jens Martensson • 1.Current diagnosis & treatment obstetrics & gynecology, 12th edition: By alan H. Decherney (author), lauren nathan (author), T. Murphy goodwin (author), neri laufer (author), ashley S. Roman (author) • 2.Obstetrics & Gynaecology Ten Teachers 19th Edition • by Philip N. Baker (Editor), Louise Kenny (Editor), Ash Monga (Editor), Stephen Dobbs (Editor) • 3.Internate: • Physiological changes of pregnancy https://medschool.ucsd.edu/som/.../Physiological%20changes%20of%20pregnancy.pp • Physiologic Changes in Pregnancy - UNC School of Medicine www.med.unc.edu/obgclerk/resources/repro-med.../PhysiologicChanges_2009.ppt • Physiological changes in pregnancy-site.iugaza.edu.ps/abahri/files/2010/.../ch-14-Physiological- changes-in-pregnancy1.pp... REFERENCE