
Recommended
Recommended
More Related Content
Similar to IPCR for cancer.pdf
Similar to IPCR for cancer.pdf (20)
Recently uploaded
Recently uploaded (20)
IPCR for cancer.pdf
- 1. Accepted Manuscript Application of immuno-PCR for the detection of early stage cancer Amjad Hayat Khan, Esmaeil Sadroddiny PII: S0890-8508(16)30010-X DOI: 10.1016/j.mcp.2016.01.010 Reference: YMCPR 1192 To appear in: Molecular and Cellular Probes Received Date: 5 December 2015 Revised Date: 29 January 2016 Accepted Date: 29 January 2016 Please cite this article as: Khan AH, Sadroddiny E, Application of immuno-PCR for the detection of early stage cancer, Molecular and Cellular Probes (2016), doi: 10.1016/j.mcp.2016.01.010. This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
- 2. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT Application of Immuno-PCR for the detection of early stage cancer Amjad Hayat Khan, Esmaeil Sadroddiny* Department of Medical Biotechnology, School of Advanced Technologies in Medicine, International Campus, Tehran University of Medical Sciences, Tehran, Iran *Corresponding Author: Dr. Esmaeil Sadroddiny, Ph.D, Department of Medical Biotechnology, School of Advanced Technologies in Medicine, Tehran University of Medical Sciences, No 88 Italia st. Tehran, Iran Email: sadroddiny@sina.tums.ac.ir PO Box. 1417755469 Tel: +98 21 88991118-24 Fax: +98 21 88991117
- 3. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT Abstract Cancer detection in premalignant stage is directly related with increase survival rate. Several biomarkers have been investigated and characterized for monitoring changes inside the cancerous cells. Although enzyme-linked immunosorbent assay (ELISA) is the method of choice in clinical practice for detecting biomarkers in serum/urine samples. However, in certain malignancies the amount of biomarkers before reaching metastasis, are too low to be detected by conventional ELISA. The seminal work of Sano et al. led to the development of highly sensitive and powerful detection method, the immuno-PCR (iPCR), which can detect very small amount of antigens/biomarkers. In spite of, several publications on iPCR sensitivity, it has not been recommended for clinical use and is limited to the scientific community only. In order to evaluate the importance of iPCR, we have made an effort to collect published studies, supporting the use of iPCR in detecting premalignant cancer. Keywords: Early cancer detection, Biomarker, Cancer screening, Immuno-PCR, Immuno- polymerase chain reaction
- 4. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT 1. Introduction According to the National Cancer Institute, North American Association of Central Cancer Registries, and National Centre for Health Statistics, cancer is the leading cause of death throughout the world [1]. Cell division, growth, and differentiation get out of control in malignancy, resulting in the development of mass of cells called tumor, except in some types of leukemia. Sometime cancerous cells disseminate from the neoplasm and spread in blood stream, thereby, leading to the formation of secondary tumors, known as metastasis. Numerous FDA approved therapeutic antibodies are available on the market for addressing diverse malignancies. However, saying that the available antibody-based therapeutics are completely safe is still under debate [2]. Therefore, patients receiving treatment need thorough surveillance and follow-up for monitoring recurrence of the disease or adverse events associated with therapy. Compromised physiological activity of cancerous cells produces certain protein antigens that are used as biomarkers in detecting malignancy. But in some types of malignancy biomarkers are produced in trace amount and more than 60% cancer patients do not show any clinical manifestations prior metastasis. After invading the surrounding cells, tissues, and/or organs; even the most effective therapeutics become least effective. Consequently, cancer diagnosis at the preliminary stage is challenging, entailing sophisticated diagnostic methods. Mutant genes sequence, their expression level, and protein structure or function is associated with malignancies. During malignancy tumor cells discharge their nucleic acid into the blood stream following apoptosis, resulting in elevated levels of circulating DNA, mRNA, and microRNA in patient’s blood. Hence, circulating cell-free DNA could be used for diagnosing early stage cancer [3, 4]. Despite of a number of reported genomic methods for cancer detection, very few of them are reliable and used in clinical settings [5]. On the other hand, protein biomarkers which are used more frequently, because scores of detection approaches have expanded their use in research laboratories. Likewise production of antigen specific antibodies has further aided in their use. Approximately, 1261 malignancy-specific protein biomarkers have been reported that express differentially in diverse types of cancer [6]. Nevertheless, very few of them are used in detecting cancer in premalignant stage. Only 9 of these proteins have been approved by FDA as “tumor associated antigens”. Discovery and validation of new biomarker candidates would help in filling up the gap between basic research and clinical use of advanced diagnostics.
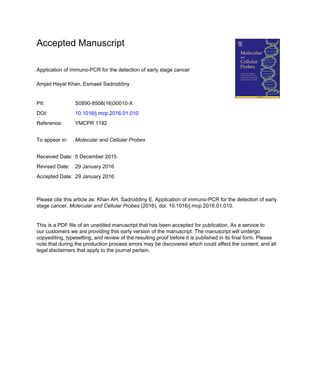
- 5. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT A large number of analytical and clinical studies have used immunoassays and now they have become the most powerful and sensitive diagnostic methods both in research and diagnostic laboratories [7]. Enzyme-linked immunosorbent assay (ELISA), is the most frequently used technique amongst immunoassays. It is reliable, effective, and sensitive for the detection and screening of target biomarkers and other antigens. Yet, some biomarkers are expressed at very small quantity that’s why their quantification is beyond the detection limit of ELISA. To obviate this major left over impediment, Sano et al. in 1992 [8], developed and introduced a fast and elegant assay, known as immuno-PCR (iPCR), in which a detection antibody is coupled with a reporter DNA. Detection antibody recognizes and binds the target biomarker, after which the conjugated-DNA fragment is amplified through PCR. This technique is 1000-fold more sensitive than the conventional ELISA and can detect even a single antigen molecule [9]. Furthermore, it has also been shown that iPCR is valuable for the detection of target antigens at large quantitative differences while ELISA, which gives a linear amplification and end point detection, is more suitable for detection of smaller differences at lower concentrations [10]. To increase the efficacy and sensitivity of this technique, iPCR protocol was assembled in different formats by bringing some improvements in the classical design (FIGURE 1). For example, DNA-directed immobilization of proteins was carried out in order to enhance the sensitivity of iPCR [11]. This modified immunoassay can be performed in a single step, thereby, reducing handling time and cost of analysis. Further advancement in iPCR technique for making the signal detection process more convenient, led to the development of real-time iPCR. This detection method is superior over the iPCR, because it quantify the target antigen and interpret results soon, as the PCR reaction proceeds. Although real-time iPCR was more accurate and precise, but it is relatively infantile as compared to the real-time PCR and iPCR, entailing validation and standardization. However, it has been used for the detection of a wide range of analytes including, viral antigens and pathologic proteins [12]. Applications of iPCR for the detection of infection has extensively been discussed and tabularized [13]. Another fascinating and worth noticing format is the phage-based open-sandwich iPCR, which was devised and for the detection of small antigen molecules i.e. human osteocalcin fragment peptide and 17β- estradiol [14]. In classical iPCR assays antibody DNA conjugation take place, either through chemicals or streptavidine-biotin system. Conversely, in phage-based open-sandwich iPCR, recombinant phages play dual role i.e. act both as antibody and DNA template, because they
- 6. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT contain antibody gene and display the corresponding gene on their surface. Hence, overcoming the need of antibody-DNA conjugation process. Furthermore, making phages is easy and they can be stored for long time in glycerol at -800 C. A slightly different approach termed, open- sandwich immunoassay has also been proposed for the quantification of low molecular weight antigens [15]. The limit of detection was 100 fg/mL, which could be increased further by optimizing the reaction conditions. In one other study a modified form of iPCR named “Multiple Simultaneous Tag (MUSTag)” was used for the detection of α-galactosidase A protein both in serum and plasma of patients, who were suffering from Fabry disease [16]. Malou and Raoult [13], reviewed the evolution iPCR from its classical format to a reliable and standardized method with the aim of overcoming the limitations in its old version. Along with iPCR, other immunoassay platforms including, Single Molecule Counting and Single Molecule Arrays have also been reported for addressing sensitivity needs [17]. Regardless of the potential sensitivity of iPCR, none of its format has been marked as a reliable and standardized detection approach. In fact, few bottlenecks including, costly reagents, complicated protocols, extended analysis time, and background signals due to non-specific binding which may lead to false-positive results limit the use of iPCR in clinical laboratories [18, 19]. Still numerous publications have persuasively witnessed the significant role of iPCR in detecting low amount of antigens/biomarkers in serum/plasma for diagnosing a variety of diseases. In current review, we discussed the application of iPCR for the detection of initial stage cancer, comparing its efficiency and sensitivity with conventional ELISA (TABLE 1). 2. Types of malignancies 2.1. Gastric cancer According to the China National Central Cancer Registry the incidence of gastric cancer is increasing both in the rural and urban areas of China [20, 21]. Presently, gastric cancer is either diagnosed through endoscopy and/or X-rays based-barium meal examination. Although endoscopy is more reliable diagnostic method; however, it is limited only to the metastatic gastric cancer patients. Initial stage gastric cancer patients are mostly asymptomatic and showing no clinical manifestation [22]. A number of biomarkers including, carcinoembryonic antigen (CEA), cancer antigen 19-9 (CA19-9), CA 72-4 and alpha-fetoprotein have been evaluated for detecting gastric cancer. Among which CA 72-4 is considered an ideal biomarker in gastric cancer [23]. In one other study monoclonal gastric cancer-7 antigen (MG7-Ag), was discovered
- 7. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT and presented as a promising gastric cancer marker with enhanced sensitivity and specificity. Immunohistochemistry tests revealed that MG7-Ag expressed more frequently in gastric cancer tissues than normal mucosa and benign lesion [24]. But unfortunately, detection of tissue MG7- Ag needs gastric biopsy which is done through endoscopy. Its expression was also observed in serum of precancerous gastric patients and may be used as a serum biomarker for the early detection gastric cancer. However, the amount of this biomarker is too low to be detected by the already established methods; therefore, iPCR was employed. MG7-Ag was measured both with iPCR and immunoradiometric assay (IRMA), and their sensitivities were compared. The former one was 33% ultrasensitive than the latter one. The DNA bands of patients with metastasis were denser on agarose gel than those without metastasis, indicating that the level of MG7-Ag was more in patients with metastasis. Hence, iPCR could be utilized for monitoring circulating tumor-associated antigens in serum after gastrectomy and observing recurrence or metastasis [22, 25]. Although iPCR was quite sensitive but still gave negative results when used for the detection of Mg7-Ag in gastric cancer patients, and the reason for lack of sensitivity was not clear. However, characterization of MG7-Ag and fine-tuning iPCR format would eliminate the impediments and improve the sensitivity and efficacy. 2.2. Prostate cancer Epidemiological studies on prostate cancer [26], have shown that since the last two decades the incidence of prostate cancer among men has tremendously increased worldwide, especially in Europe. This increase in incidence is directly related with age and can be cured markedly; if, restricted to the prostate; otherwise, metastatic one is difficult to cure. A study conducted on prostate cancer patients showed that the mortality rate due to prostate cancer is 13000 each year. Undoubtedly, early diagnosis of the disease may reduce the risk of progression and malignancy. Prostate specific antigen (PSA), a renowned biomarker has extensively been used in detecting prostate cancer. Yet, false positive and false negative results have been observed. PSA related indexes including, PSA density, age-adjusted PSA, and percent free PSA could enhance the positive predicting value of PSA-testing [27, 28]. The amount of PSA above the cut-off value (2.5-4.0 ng/mL) is commonly considered as PSA positive and the patient may need biopsy. Therefore, ultrasensitive detection assays are needed to quantify PSA level below the cut-off value i.e. in pg/mL and facilitate the earlier detection of the disease. In case of prostatectomy the PSA should be undetectable; otherwise, trace amount of PSA may be considered as the
- 8. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT recurrence of the disease. To quantify PSA even in trace amount, iPCR was assembled in various formats to increase the sensitivity. Quantification results of three approaches were compared with each other and with conventional ELISA. Based on the use of same antibodies, the sensitivity of real time iPCR was high as compared to conventional ELISA. The ultra-sensitivity of the iPCR is attributed to the signal generation and detection processes. In ELISA the detection antibody is attached with the detection system that gives linear signal increase with time while in iPCR the detection antibody is part of the PCR system which produces an exponential signal growth in time. Moreover, ELISA signals readout system use intensity while in real-time PCR; the number of amplification cycles needed to reach a particular point are recorded [29]. In radical prostatectomy the rise of PSA level above 0.2 ng/mL is considered failure of the prostatectomy and recurrence of the disease [30]. Hence, ELISA cannot be used for follow-up of prostatectomic patient and monitoring recurrence of the disease. Recently, nucleic acid detection immunoassay, which is an advanced format of iPCR for the quantification of total serum PSA, has been developed. Several modification have been brought about in iPCR protocol for minimizing non- specific binding and enhancing precision. The limit of detection of nucleic acid detection immunoassay was approximately 0.27 ng/L [31]. It is obvious that iPCR is indispensible for the detection of even trance amount of PSA especially in prostatectomic patients. The introduction of ready-to-use reagents, refinement of assay protocol, and the development of commercial iPCR kits would further facilitate the detection process and pave the way for iPCR to become a routine diagnostic method. 2.3. Breast cancer In the past breast cancer was considered as the disease of the Western world. But over the past two decades the incidence of breast cancer has increased terrifically in poor countries. According to the 2008 GLOBOCAN approximations, out of the total breast cancer worldwide half have been reported in developing countries [32]. Breast cancer biomarkers including, CA 15-3, BR 27.29, CEA, tissue polypeptide antigen, tissue polypeptide specific antigen, and HER2+ (the extracellular domain) have been utilized for diagnosing breast cancer. Unluckily, the main drawback in using these biomarkers was the lack of sensitivity and gave no significant results in preliminary stage breast cancer [33]. Mammography, ultrasonography, computerized tomography, magnetic resonance imaging, positron emission tomography, and methoxyisobutylisonitrile imaging have been employed to diagnose breast cancer. Nevertheless,
- 9. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT physical examination techniques were less sensitive and unable to distinguish between benign and malignant tumors. Hence, detection of breast cancer in early stage could only be helpful in treatment and reducing the chance of metastasis. CA 15-3 along with CEA is a remarkable biomarker in breast cancer and used more frequently in detecting the disease. With the aim of developing precise and sensitive method to detect CA 15-3 in breast cancer, a carbon nanotube iPCR was developed. The lower detection limit of this method was approximately, 0.001-0.01 U/mL [34], which is extremely sensitive than the other bioanalytical assays. Actually, metastatic breast cancer spread through blood; therefore, circulating HER2+ cells could also be used as biomarkers. Site directed mutagenesis was carried out in trastuzumab Fab fragment which is used for targeting HER2+ cells for treating breast cancer. The purpose of the study was to design more sensitive and specific iPCR protocol to detect even trace amount of HER2+ cells in patients’ blood. The modified form of iPCR was able to detect extremely rare as low as 11 HER2+ cells in 1.4 million white blood cells [35]. The sensitivity of this technique was high enough and be a possible method of choice for the quantification of circulating tumor cells in blood for monitoring the recurrence of the disease and response to treatment. 2.4. Nasopharyngeal carcinoma Nasopharyngeal carcinoma (NPC), is a rare and subtype of the head and neck cancer. Environmental factors and genetic susceptibility are believed to have a role in its pathogenesis. The Epstein-Barr virus (EBV) has also been implicated as the cause of NPC [36]. A prospective cohort study conducted on NPC patients, demonstrated that immunoglobulin A (IgA) antibodies against EBV-capsid antigen and the presence of anti-EBV DNase antibodies are the most reliable biomarkers for diagnosing NPC. Increased titers of IgA antibodies against EBV-capsid antigen and anti-EBV DNase antibodies have been observed before the occurrence of NPC [37]. For early diagnosis and post-treatment observations of NPC patients; three different serological techniques have been used and compared with one another. The results revealed that ELISA method was more suitable for the diagnosing preliminary NPC and monitoring prognosis [38]. But NPC patients’ undergone radiotherapy or chemotherapy the concentration of EBV nuclear antigen in serum decreased dramatically, resulting very minute amount of antibodies titers in serum. Hence, ELISA would not be able to detect this trace amount precisely. Wang et al [39] used an updated version of iPCR to detect NPC in initial stage. Detection efficiency of glass substrate-based iPCR was compared with conventional ELISA on the base of affinity, sensitivity,
- 10. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT and specificity. Advanced format of iPCR was two-fold more sensitive than the conventional ELISA. Based on the efficiency of iPCR sensitivity, affinity, and specificity for the early detection of NPC biomarkers a kit with ready-to-use reagents has also been invented and patented [40]. This kit was able to generate the signal even when the serum was diluted 15,000- folds. Hence, it can easily discriminate between NPC patients and normal subjects. On the other hand conventional ELISA failed to detect the target protein when serum was diluted beyond 2000-folds. Patenting iPCR kit is a great achievement in detecting NPC in initial stage. 2.5. Ovarian cancer Ovary cancer is the sixth common cancer and fifth leading cause of death in women worldwide [1]. Despite many treatment options, this disease is still a major dilemma. In the last few decades there was no reliable method for the detection of ovarian cancer because its detection in the early stage was challenging. The five years survival rate of ovarian cancer patients could increase, if detected in early stage; otherwise, this rate may reduce to 30%. Heparin-binding EGF-like growth factor (HB-EGF), expressed as a membrane-anchored protein which is then cleaved to soluble active form by a process called ectodomain shedding. The released soluble active form in extracellular space is implicated in pathogenesis of ovarian cancer. Kasai et al. [41], have devised an accurate and precise iPCR method for the detection of soluble HB-EGF in human serum. Compared to the previous studies in which polyclonal antibodies were used, the detection limit of this approach was more. Moreover, this method can detect only an active form of soluble HB-EGF which is considered to be involved in the pathogenesis of the disease. While the previous techniques could detect any form of HB-EGF; hence, detection of only soluble form is more meaningful. Studies have demonstrated that epidermal growth factor-like domain 7 (EGFL7) overexpressed in ovary cancer and can be used for detecting the disease [42]. In contemplation of increasing throughput and decreasing the consumption of sample and reagents, iPCR was designed in 384-wells format to quantify EGFL7. Besides, ovarian cancer this method has the potentiality to detect EGFL7 in non-small-cell lung cancer (NSCLC), hepatocellular carcinoma (HCC) cell lines, HCC, and breast cancer. Utilizing the same antibodies iPCR was 16- folds ultrasensitive than conventional ELISA [43]. Another very sensitive marker i.e. CA 125 in ovarian cancer is also a good candidate for detecting the disease in early stage. It was originally used for observing the patients with ovarian cancer because changes in CA 125 can track the progression and regression of the disease in response to treatment accurately [44]. Based on the
- 11. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT importance of CA 125 in ovarian cancer, production of anti-CA 125 antibodies and their utilization in developing iPCR will aid in the detection of the disease in early stage. 2.6. Bone cancer Bone metastasis is found more in patients having solid tumors. Micronutrients of the bone marrow highly support the growth and nourishment of the disseminated tumor cells. These circulating tumor cells aggregate inside the bone marrow, resulting in bone metastasis that spread to other parts of the body or even reseed the original organ from which they were detached. In this way bone metastasis interrupt bone hemostasis, disturbing the phenomena of bone remodeling or bone metabolism that leads to reduced bone integrity and increased skeletal impediments. During the process of bone remodeling certain peptide biomarkers are produced, ensuring normal cellular activity. The presence of such markers in serum and urine may help the physician to monitor the risk of skeletal-related events and response of the patients to treatment [45]. A well-known cytokine, osteoprotegerin (OPG)/osteoclastogenensis inhibitory factor (OCIF), is a soluble member of tumor necrosis factor receptor family of proteins. OPG/OCIF negatively regulates osteoclast bone resorption. Two types of ELISAs have been developed: one that detect monomeric and homodimeric form of recombinant OPG/OCIF equally while the other specifically detect homodimeric form only [46]. But the concentration of homodimeric form of OPG in blood is too low to be detected by ELISA. Furuya et al [47], devised iPCR for the detection of homodimeric form of OPG in sera of both patients and normal population. To determine the detection limit of iPCR, recombinant OPG was serially diluted in various concentrations i.e. (0, 1, 2.5, 5, 10, 25, 50, and 100 pg/L). The limit of detection of iPCR for OPG was 5 pg/L. Although half-life of homodimeric form of OPG is very short as compared to the monomeric form. But studies conducted on animal models have shown that the homodimeric form exerts more biological activity in reducing calcium concentration in serum of rats than the monomeric form [48]. Therefore, determining the accurate concentration of homodimeric form of OPG is more beneficial than the monomeric form. Lower concentration of homodimeric form in serum may be due to the reason that after carrying out its role in blood either it redistributes to the tissues or degrades into monomeric form. 2.7. Colorectal carcinoma According to the National Cancer Institute’s Surveillance and National Centre for Health Statistics; colorectal cancer is the third most common cancer and the third leading cause of
- 12. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT mortality both in men and women in US. It can be treated if detected in early stage; unfortunate, 70% of the patients with this disease are diagnosed in advanced stage [49, 50]. Cyclooxygenase- 2 (Cox-2) is an inducible enzyme, converting arachidonic acid to prostaglandins, and is associated with the metastasis of colorectal cancer. Overexpression of Cox-2 is linked with colorectal cancer metastasis and has been observed in glandular cavity of colorectal cancer and interstitial tissues. For the detection of Cox-2 in the serum an improved iPCR format known as immunobead-PCR [51], was developed and used to confirm that Cox-2 is a significant biomarker in colorectal cancer. It was 100-1000-fold more sensitive than conventional ELISA. The advantage of this technique was that it can be done in a single step, thereby, reducing the handling time. False positive results have been observed which could be minimized by including positive and negative controls. In one other study it was observed that candherin-17 (CDH17), a membrane protein of serum exosomes overexpressed in colorectal cancer cells, may also be employed as a biomarker in colorectal cancer [52]. Nikitina et al [53], used microbeads-based iPCR for the detection of CDH17 in serum exosomes. The iPCR easily distinguished between the serum of healthy people and colon cancer patients. However, lager panel studies are required to establish a relation of this protocol with early stage colorectal cancer and to determine its limit of detection. 2.8. Hepatocellular carcinoma Epidemiological studies conducted on the incidence of hepatocellular carcinoma (HCC) have shown a three-folds increase in HCC since, 1975 to 2005 in US [54]. Advancement in the field of cancer biology and detection techniques has enabled the scientists to find out new biomarkers which may assist the physicians in detection and monitoring of the disease; especially, in premalignant stage. Behne and Copur [55], have reviewed in detail various tissue and serum- based biomarkers that are involved in HCC. EGFL7 biomarker expresses more frequently in tumorigenesis; therefore, its overexpression was studied in HCC cells and tissues. It was observed that overexpression of EGFL7 is linked with the poor prognosis of the disease. In vivo studies in animals reveled that EGFL7 promote cell motility by facilitating the phosphorylation of focal adhesion kinase [56]. Hence, it could be used as an ideal biomarker in the early detection of HCC. Zhang et al [43], employed real time iPCR in more advanced form to precisely quantify the level of circulating human EGFL7 which was 16-times more sensitive than ELISA. Alpha- fetoprotein (AFP) is an embryonic protein, expressed in the mesenchymal cells in the fetal liver
- 13. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT and yolk cells. After birth of the baby the expression of AFP stops and the protein is removed from the body. Metastasis in hepatocytes twitches the expression of AFP, resulting in an elevated level of this protein in peripheral blood [57]. Consequently, AFP could also serve as a biomarker in the early detection of HCC. Production of antibodies against AFP would pave the way towards the design of iPCR method, thereby, enhancing the detection process of HCC. 3. Discussion In the past few decades several types of malignancy have been recognized which are the leading cause of death throughout the world. Numerous studies have shown that cancer patients produce protein biomarkers which are particularly well-suited for discriminating cancer patients from healthy subjects and can be used for the detection and classification of cancer. Highly efficient and ultrasensitive protein detection methods have aided the detection of cancer, control, surveillance, and treatment program. Unluckily, cancerous cells in a number of malignancies express biomarkers in trace amount before reaching metastasis; thereby, constraining the physicians to detect the disease in early stage. For the quantification of cancer biomarkers various immunoassays have been employed, among which ELISA is the most widely used due to its sensitivity and throughput. But certain proteins; such as, cytokines and kinases carry out their tasks in trace amount. Hence, their detection is beyond the threshold limit of ELISA [59]. An advanced and versatile technique, iPCR was developed which is a powerful method for detecting target proteins. In iPCR, an oligonucleotide sequence is coupled with a biomarker specific antibody. The detection antibody binds with the antigen while signal is generated by amplifying the attached oligonucleotide sequence through PCR [8]. This method can detect up to 15 femtograms (10-19 moles) of antigen molecules and is considered perfect for the detection of trace amount of antigens in complex biological samples [9]. Still there is a lot of room to modify the technique by introducing various formats and assemblages to the classical format. Published studies have revealed that changes carried out in iPCR have amplified the sensitivity and detection limit [29]. However, certain factors such as, complicated multistep protocols, expensive reagents, expertise, and high background signals limit its use in clinical application. In addition, DNA-antibody conjugates if not prepared properly or contaminated with free binding proteins or marker DNA, may lead to background signals in iPCR [19]. Despite of these limiting factors, iPCR has successfully been used for the detection of low concentration of plethora of cancer-associated biomarker candidates. Problems regarding complicated multistep protocols
- 14. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT were solved by using real-time PCR, which overwhelmed the burden of detecting reporter DNA on gel, thus reducing the time of detection and risk of false positive results. Additionally, high background signals can be reduced by proper blocking protocols. The use of specific antibodies with high affinity, and efficient coupling of antibodies with reporter DNA could be helpful in modifying iPCR assay [18]. Furthermore, when the data from iPCR are used to diagnose the cancers, the calculation method i.e. using 4-parameters logistic non-linear regression model and statistical significance is much more important [16]. A number of published data supported the notion that further manipulation of iPCR and ready to use reagents will make it an ideal technique for the detection of early stage cancer. Several modified iPCR assays are commercially available in USA, Japan and EU countries; however, unluckily, there are a few cases available in clinical situation. We anticipate that in near future, iPCR kits for detection of diverse biomarkers would continue to march on the market for the early detection of malignancies, infections, and for the detection of contaminants in food and other products. 4. Conclusion We conclude that iPCR is highly sensitive in detecting lower concentration of biomarkers. Based on its powerful potential and progress from its classical format to more advanced formats with ready to use reagents, we could say that it will become a reference detection method in near future. Conflict of interest: This review is the outcome of financially non-supported in house study and the authors declare no conflict of interest. References: 1. R. Siegel, J. Ma, Z. Zou, A. Jemal, Cancer statistics, 2014, CA Cancer J Clin. 64 (2014) 9-29. 2. A.H. Khan, E. Sadroddiny, Licensed monoclonal antibodies and associated challenges, Hum Antibodies. 23 (2015) 63-72. DOI 10.3233/HAB-150286. 3. G. Sozzi, D. Conte, M. Leon, R. Ciricione, L. Roz, C. Ratcliffe, et al., Quantification of free circulating DNA as a diagnostic marker in lung cancer, J Clin Oncol. 21 (2003) 3902-8.
- 15. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT 4. Y.I. Elshimali, H. Hhaddour, M. Sarkissyan, Y. Wu, J.V. Vadgama, The clinical utilization of circulating cell free DNA (CCFDNA) in blood of cancer patients, Int J Mol Sci. 14 (2013) 18925-58. 5. D. Sidransky, Emerging molecular markers of cancer, Nat Rev Cancer. 2 (2002) 210-219. 6. M. Polanski, N.L. Anderson, A List of Candidate Cancer Biomarkers for Targeted Proteomics, Biomark Insights. 1 (2006) 1-48. 7. R.M. Lequin, Enzyme immunoassay (EIA)/enzyme-linked immunosorbent assay (ELISA), Clin Chem. 51 (2005) 2415-8. 8. T. Sano, C. Smith, C. Cantor, Immuno-PCR: very sensitive antigen detection by means of specific antibody-DNA conjugates, Science. 258 (1992) 120-122. 9. C.M. Niemeyer, M. Adler, D. Blohm, Fluorometric polymerase chain reaction (PCR) enzyme-linked immunosorbent assay for quantification of immuno-PCR products in microplates, Anal Biochem. 246 (1997) 140-145. 10. L. Potůčková, F. Franko, M. Bambousková, P. Dráber, Rapid and sensitive detection of cytokines using functionalized gold nanoparticle-based immuno-PCR, comparison with immuno-PCR and ELISA, J Immunol Methods. 371 (2011) 38-47. 11. C.M. Niemeyer, R. Wacker, M. Adler, Combination of DNA-directed immobilization and immuno-PCR: very sensitive antigen detection by means of self-assembled DNA- protein conjugates, Nucleic Acids Res. 31 (2003) e90. DOI: 10.1093/nar/gng090. 12. J. Barletta, Applications of real-time immuno-polymerase chain reaction (rt-IPCR) for the rapid diagnoses of viral antigens and pathologic proteins, Mol Aspects Med. 27 (2006) 224-253. 13. N. Malou, D. Raoult, Immuno-PCR: a promising ultrasensitive diagnostic method to detect antigens and antibodies, Trends Microbiol. 19 (2011) 295-302. 14. J. Dong, S. Hasan, Y. Fujioka, H. Ueda, Detection of small molecule diagnostic markers with phage-based open-sandwich immuno-PCR, J Immunol Methods. 377 (2012) 1-7. 15. S. Hasan, J. Dong, Y. Hara, Y. Morizane, F. Shibasaki, H Ueda, Protein-based open sandwich immuno-PCR for sensitive detection of small biomarkers, Anal Sci. 29 (2013) 871-876.
- 16. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT 16. S. Nakano, Y. Morizane, N. Makisaka, T. Suzuki, T. Togawa, T. Tsukimura et al., Development of a Highly Sensitive Immuno-PCR Assay for the Measurement of α- Galactosidase A Protein Levels in Serum and Plasma, PLoS One. 8 (2013) e78588. 17. S.K. Fischer, A. Joyce, M. Spengler, T.Y. Yang, Y. Zhuang, M.S. Fjording, et al., Emerging technologies to increase ligand binding assay sensitivity, AAPS J. 17 (2015) 93-101. 18. N. Malou, A. Renvoise, C. Nappez, D. Raoult, Immuno-PCR for the early serological diagnosis of acute infectious diseases: the Q fever paradigm, Eur J Clin Microbiol Infect Dis. 31 (2012) 1951-60. 19. C.M. Niemeyer, M. Adler, R. Wacker, Immuno-PCR: high sensitivity detection of proteins by nucleic acid amplification, Trends Biotechnol. 23 (2005) 208-16. 20. W. Chen, R. Zheng, S. Zhang, P. Zhao, G. Li, L. Wu, J. He, Report of incidence and mortality in China cancer registries, 2009, Chin J Cancer Res. 25 (2013) 10-21. 21. Y. Yuan, A survey and evaluation of population-based screening for gastric cancer, Cancer Biol Med. 10 (2013) 72-80. 22. J. Ren, Z. Chen, S.J. Juan, X.Y. Yong, B.R. Pan, D.M. Fan, Detection of circulating gastric carcinoma-associated antigen MG7-Ag in human sera using an established single determinant immuno-polymerase chain reaction technique, Cancer. 88 (2000) 280-285. 23. R. Mattar, C.R. Alves de Andrade, G.M. DiFavero, J.J. Gama-Rodrigues, A.A. Laudanna, Preoperative serum levels of CA 72-4, CEA, CA 19-9, and alpha-fetoprotein in patients with gastric cancer, Rev Hosp Clin Fac Med Sao Paulo. 57 (2002) 89-92. 24. J. Liu, J.L. Hu, X.Y. Zhang, T.D. Qiao, X.T. Chen, K.C. Wu, et al., The value of MG7 antigen in predicting cancerous change in dysplastic gastric mucosa, Int J Clin Pract. 56 (2002) 169-72. 25. L. Zhang, J. Ren, K. Pan, J. Ma, J. Li, L. Shen, et al., Detection of gastric carcinoma- associated MG7-Ag by serum immuno-PCR assay in a high-risk Chinese population, with implication for screening, Int J Cancer. 126 (2010) 469-473. 26. F. Bray, J. Lortet-Tieulent, J. Ferlay, D. Forman, A. Auvinen, Prostate cancer incidence and mortality trends in 37 European countries: An overview, Eur J Cancer. 46 (2010) 3040-3052.
- 17. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT 27. H. Luboldt, H. Rübben, PSA-based early detection of prostate cancer, Der Urologe. Ausg. A. 39 (2000) 22-26. 28. D.A. Healy, C.J. Hayes, P. Leonard, L. McKenna, R. O'Kennedy, Biosensor developments: application to prostate-specific antigen detection, Trends Biotechnol. 25 (2007) 125-131. 29. K. Lind, M. Kubista, Development and evaluation of three real-time immuno-PCR assemblages for quantification of PSA, J Immunol Methods. 304 (2005) 107-116. 30. E.J. Vassilikos, H. Yu, J. Trachtenberg, R.K. Nam, S.A. Narod, I.L. Bromberg, et al., Relapse and cure rates of prostate cancer patients after radical prostatectomy and 5 years of follow-up, Clin Biochem. 33 (2000) 115-23. 31. J.E. McDermed, R. Sanders, S. Fait, R.E. Klem, M.J. Sarno, T.H. Adams, et al., Nucleic acid detection immunoassay for prostate-specific antigen based on immuno-PCR methodology, Clin Chem. 58 (2012) 732-40. 32. J. Ma, A. Jemal, Breast Cancer Statistics, in Breast Cancer Metastasis and Drug Resistance, A. Ahmad, Editor., Springer New York, 2013, pp. 1-18. 33. M.J. Duffy, Serum tumor markers in breast cancer: are they of clinical value? Clin Chem. 52 (2006) 345-351. 34. S. Sadhasivam, J.C. Chen, S. Savitha, C.W. Chang, F.H. Lin, Application of carbon nanotubes layered on silicon wafer for the detection of breast cancer marker carbohydrate antigen 15-3 by immuno-polymerase chain reaction, J Mater Sci Mater Med. 25 (2014) 101-111. 35. S.A. Kazane, D. Sok, E.H. Cho, M.L. Uson, P. Kuhn, P.G. Schultz, et al., Site-specific DNA-antibody conjugates for specific and sensitive immuno-PCR, Proc Natl Acad Sci U S A. 109 (2012) 3731-3736. 36. J. Chou, Y.C. Lin, J. Kim, L. You, Z. Xu, B. He, et al., Nasopharyngeal carcinoma-- review of the molecular mechanisms of tumorigenesis, Head Neck. 30 (2008) 946-63. 37. Y.C. Chien, J.Y. Chen, M.Y. Liu, H.I. Yang, M.M. Hsu, C.J. Chen, et al., Serologic Markers of Epstein–Barr Virus Infection and Nasopharyngeal Carcinoma in Taiwanese Men, N Engl J Med. 345 (2001) 1877-1882. 38. H. Karray, W. Ayadi, L. Fki, A. Hammami, J. Daoud, M.M. Drira, et al., Comparison of three different serological techniques for primary diagnosis and monitoring of
- 18. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT nasopharyngeal carcinoma in two age groups from Tunisia, J Med Virol. 75 (2005) 593- 602. 39. T.W. Wang, H.Y. Lu, P.J. Lou, F.H. Lin, Application of highly sensitive, modified glass substrate-based immuno-PCR on the early detection of nasopharyngeal carcinoma, Biomaterials. 29 (2008) 4447-4454. 40. H.Y. Lu, T.W. Wang, F.H. Lin, P.J. Lou, Immuno-PCR method for detecting nasopharyngeal carcinoma markers and kit thereof, 2010, Google Patents. 41. N. Kasai, K. Kobayashi, S. Shioya, Y. Yoshikawa, F. Yotsumoto, S. Miyamoto, et al., Soluble heparin-binding EGF-like growth factor (HB-EGF) detected by newly developed immuno-PCR method is a clear-cut serological biomarker for ovarian cancer, Am J Transl Res. 4 (2012) 415-421. 42. J. Oh, S.H. Park, T.S. Lee, H.K. Oh, J.H. Choi, Y.S. Choi, High expression of epidermal growth factor-like domain 7 is correlated with poor differentiation and poor prognosis in patients with epithelial ovarian cancer, J Gynecol Oncol. 25 (2014) 334-41. 43. J. Zhang, J.M. Vernes, J. Ni, C. Nelson, A. Wong, S.T. Chen, et al., Real-time immuno- polymerase chain reaction in a 384-well format: Detection of vascular endothelial growth factor and epidermal growth factor-like domain 7, Anal Biochem. 463 (2014) 61-66. 44. L.E. Moore, R.M. Pfeiffer, Z. Zhang, K.H. Lu, E.T. Fung, R.C. Bast Jr, Proteomic biomarkers in combination with CA 125 for detection of epithelial ovarian cancer using prediagnostic serum samples from the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial, Cancer. 118 (2012) 91-100. 45. R. Coleman, J. Brown, E. Terpos, A. Lipton, M.R. Smith, R. Cook, et al., Bone markers and their prognostic value in metastatic bone disease: Clinical evidence and future directions, Cancer Treat Rev. 34 (2008) 629-639. 46. K. Yano, E. Tsuda, N. Washida, F. Kobayashi, M. Goto, A. Harada, et al., Immunological Characterization of Circulating Osteoprotegerin/Osteoclastogenesis Inhibitory Factor: Increased Serum Concentrations in Postmenopausal Women with Osteoporosis, J Bone Miner Res. 14 (1999) 518-527. 47. D. Furuya, R. Kaneko, A. Yagihashi, T. Endoh, T. Yajima, D. Kobayashi, et al., Immuno-PCR assay for homodimeric osteoprotegerin, Clin Chem. 47 (2001) 1475-1477.
- 19. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT 48. A. Tomoyasu, M. Goto, N. Fujise, S. Mochizuki, H. Yasuda, T. Morinaga, et al., Characterization of monomeric and homodimeric forms of osteoclastogenesis inhibitory factor, Biochem Biophys Res Commun. 245 (1998) 382-7. 49. R. Siegel, C. DeSantis, A. Jemal, Colorectal cancer statistics, 2014, CA Cancer J Clin. 64 (2014) 104-117. 50. O.K. Bernhard, D.W. Greening, T.W. Barnes, H. Ji, R.J. Simpson, Detection of cadherin- 17 in human colon cancer LIM1215 cell secretome and tumour xenograft-derived interstitial fluid and plasma, Biochim Biophys Acta. 1834 (2013) 2372-9. 51. L.G. Li, X.Y. Wang, J.L. Chang, W.B. Xie, T.F. Liu, Q.L. Zhang, et al., The establishment of supramolecular immunobead real-time PCR and the identification of Cox-2 as a metastasis-related marker in colorectal carcinoma, Oncol Rep. 28 (2012) 977- 984. 52. R.A. Bartolome, R. Barderas, S. Torres, M.J. Fernandez-Aceñero, M. Mendes, J. García- Foncillas, et al., Cadherin-17 interacts with alpha2beta1 integrin to regulate cell proliferation and adhesion in colorectal cancer cells causing liver metastasis, Oncogene. 33 (2014) 1658-69. 53. I.G. Nikitina, E.Y. Sabirova, O.N. Solopova, S.A. Surzhikov, E.N. Grineva, V.L. Karpov, et al., A new immuno-PCR format for serological diagnosis of colon cancer, Mol Biol. 48 (2014) 99-104. 54. S.F. Altekruse, K.A. McGlynn, M.E. Reichman, Hepatocellular carcinoma incidence, mortality, and survival trends in the United States from 1975 to 2005. J Clin Oncol. 27 (2009) 1485-1491. 55. T. Behne, M.S. Copur, Biomarkers for hepatocellular carcinoma, Intl J Hepatol. 2012 (2012). doi:10.1155/2012/859076. 56. F. Wu, L.Y. Yang, Y.F. Li, D.P. Ou, D.P. Chen, C. Fan, Novel role for epidermal growth factor-like domain 7 in metastasis of human hepatocellular carcinoma, Hepatology. 50 (2009) 1839-1850. 57. Y.K. Huang, X.G. Fan, F. Qiu, Z.M. Wang, Combined detection of mRNA expression of Alpha-fetoprotein in peripheral blood and telomerase activity of monocytes in hepatocellular carcinoma patients, Hepatogastroenterology. 60 (2013) 1-5.
- 20. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT 58. R. Jun, D.M. Fan, S.J. Zhou, Establishment of immuno-PCR technique for the detection of tumor associated antigen MG7-Ag on the gastric cancer cell line, Chin J Cancer Res. 7 (1995) 247-250. 59. E.A. Wayner, S.I. Quek, R. Ahmad, M.E. Ho, M.A. Loprieno, Y. Zhou, et al., Development of an ELISA to detect the secreted prostate cancer biomarker AGR2 in voided urine, Prostate. 72 (2012) 1023-1034.
- 21. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT Table 1. Comparison of limit of detection of iPCR with conventional ELISA/other immunoassays for detecting biomarkers in preliminary stage cancer Biomarkers Limit of detection of iPCR Limit of detection of ELISA/other immunoassay Reference PSA 4.8×105 PSA molecules ˜0.2 pg/mL 5.7×107 PSA molecules [29] CA 15-3 0.001-0.01 U/ml 15 U/mL [34] HER2+ cells 11 cells out of 1.4 million WBCs - [35] IgA antibodies against EBV capsid antigen, Anti-EBV DNase antibodies Serum dilution range upto15,000-folds Serum dilution range up to 2,000-folds [40] HB-EGF 100-5.0 pg/mL 0.34 ng/mL [41] EGFL7 0.51 pM 8.2 pM [43] OPG 5.0 fg/mL 65 pg/mL [46] MG-7 Ag 3.8×10-14 moles 3.0×10-11 moles [58]
- 22. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT Figure 1. A. Classical iPCR format: An antigen specific mAb is immobilized on the surface of microtiter plate and free binding sites on the plate are blocked with blocking reagents. Antigen is added to the well which binds to the captured mAb. Streptavidin (STV) conjugated with biotinylated oligonucleotide and biotinylated detection mAb is added. mAb binds with the target antigen after which the signal is generated by amplifying the conjugated oligonucleotide through PCR. B. Microbeads based-iPCR: mAb is captured on the surface of microtiter plate and blocking is done. After adding antigen, then microbeads to which the detection antibody and reporter DNA are attached are added. Finally, oligonucleotide is amplified using PCR. C. DNA directed immobilization: In this format STV which contains a biotinylated ssDNA is coated on the surface of microtiter plate. A preconjugate of STV, containing a biotinylated ssDNA that is complementary to the surface-immobilized ssDNA and biotinylated mAb is added. Complimentary ssDNAs hybridize with each other. Immobilized mAb then binds with the antigen and finally the signal is generated by iPCR, using oligomeric conjugates of STV bis- biotinylated dsDNA and biotinylated mAb. The read-out of iPCR is carried out using real-time PCR [11]. Microbead B Streptavidin Biotin Reporter DNA Antigen A C STV+bis-biotinylated dsDNA+bis-biotinylated mAb STV+biotinylated ssDNA+biotinylated mAb
- 23. M A N U S C R I P T A C C E P T E D ACCEPTED MANUSCRIPT 1. Immuno-PCR is proposed for detection of early stage cancer 2. Early detection of cancer significantly reduces the mortality rate 3. Immuno-PCR is more sensitive than ELISA for the detection of trace amount of biomarkers