Download to read offline




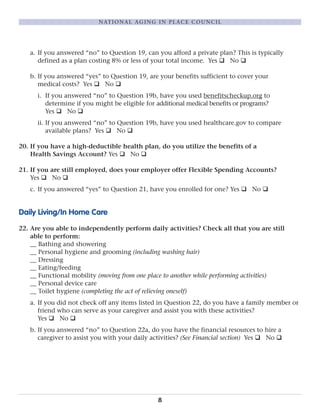

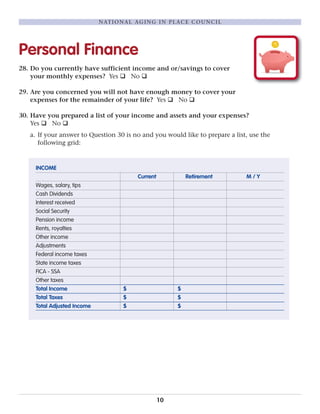

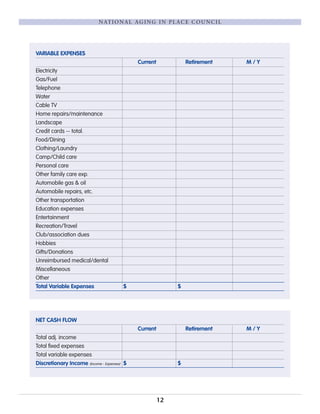






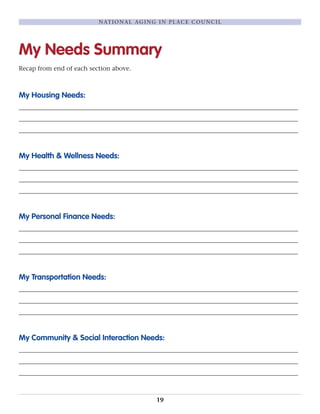


The document provides a questionnaire to help assess needs for aging in place. It addresses housing, health, finances, transportation, and community/social needs. The housing section asks about comfort and affordability of current residence and preferences. The health section asks about medicare/insurance coverage, daily living abilities, and legal planning. The finance section asks about income, expenses, benefits, and planning tools. The transportation section asks about driving ability and alternative transportation options. The social section asks about social interaction and support systems. The goal is to help individuals identify any needs and resources to help them continue living independently.















































