
Recommended
Recommended
More Related Content
Similar to Fetal aortic valvuloplasty prevents HLHS
Similar to Fetal aortic valvuloplasty prevents HLHS (20)
Recently uploaded
Recently uploaded (20)
Fetal aortic valvuloplasty prevents HLHS
- 1. R E V I E W A R T I C L E Fetal aortic valvuloplasty to prevent progression to hypoplastic left heart syndrome in utero Matthew A. Crystal | Lindsay R. Freud Department of Pediatrics, Division of Pediatric Cardiology, Columbia University Medical Center, Morgan Stanley Children's Hospital of NewYork- Presbyterian, New York, New York Correspondence Lindsay R. Freud, MD, Department of Pediatrics, Division of Pediatric Cardiology, Columbia University Medical Center, Morgan Stanley Children's Hospital of NewYork-Presbyterian, 3959 Broadway, Children's Hospital North, 2nd Floor, New York, NY 10032. Email: lrf2136@columbia.edu Advances in fetal echocardiography have allowed for the prenatal diagnosis of con- genital heart disease and an understanding of its natural history in utero. This insight has led to the development of fetal cardiac intervention (FCI) for select defects to prevent significant morbidity or mortality postnatally. Fetal aortic valvu- loplasty (FAV) may be performed to prevent progression to hypoplastic left heart syndrome, a severe form of congenital heart disease, in utero. The current review focuses on this type of FCI and discusses the history of FAV, the rationale for intervention, candidate selection, procedural technique, and outcomes to date. Finally, the importance of building a multidisciplinary team to perform FCI is addressed. KEYWORDS congenital heart disease, fetal cardiac intervention, fetal echocardiography, hypoplastic left heart syndrome, prenatal diagnosis 1 | INTRODUCTION Fetal echocardiography allows for the early detection of con- genital heart defects. A small subset of defects may progress in severity before birth. Percutaneous fetal cardiac interven- tion (FCI) was developed in an attempt to modify the natural history of these lesions. One of the most well-described defects is severe, mid- gestation aortic stenosis (AS), which may progress to hypo- plastic left heart syndrome (HLHS) by the time of birth. Staged univentricular surgical palliation has allowed chil- dren with HLHS to survive with the right ventricle acting as the systemic ventricle, but significant issues related to peri- operative mortality, long-term morbidity, and neurodevelop- mental disability remain (Ghanayem et al., 2012; Mitchell et al., 2006; Williams et al., 2009). Fetal aortic valvuloplasty (FAV) is performed to prevent evolution to HLHS and, ide- ally, to allow children to have a biventricular circulation. Maxwell, Allan, and Tynan first performed FAV in 1991. Although technical success was achieved in one of the two fetuses in their report, there were challenges regarding optimal patient selection and procedural technique (Maxwell, Allan, & Tynan, 1991). After another decade, the global expe- rience of FAV reached only 12 reported cases (Kohl, Sharland et al., 2000). Greater success was ultimately achieved in the 2000's due to a better understanding of the natural history, which allowed for refinement of patient selection, and techni- cal modifications. Over the past decade, FAV has become more widespread; however, it is still largely performed at major academic medical centers with expertise in fetal cardi- ology, catheterization, and high-risk obstetrics. 2 | RATIONALE FOR INTERVENTION AND PATIENT SELECTION Multiple natural history studies have demonstrated that fetuses with severe AS at mid-gestation commonly evolve to HLHS by the time of birth (Allan, Sharland, & Tynan, 1989; Danford & Cronican, 1992; McCaffrey & Sherman, 1997; Simpson & Sharland, 1997). In the presence of severe AS, left ventricular (LV) dilation and dysfunction occur. As the LV becomes less capable of supporting the circulation, sev- eral additional pathophysiologic features develop, including monophasic mitral inflow, left to right flow at the foramenThe authors have no financial disclosures to report. Received: 29 January 2019 Accepted: 30 January 2019 DOI: 10.1002/bdr2.1478 Birth Defects Research. 2019;1–6. wileyonlinelibrary.com/journal/bdr2 © 2019 Wiley Periodicals, Inc. 1
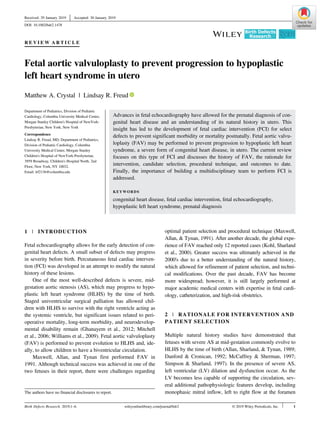
- 2. ovale, and flow reversal in the transverse aortic arch. These features may be used to select fetuses that are likely to evolve to HLHS by the time of birth and are, therefore, potential candidates for FAV (Makikallio et al., 2006). Tech- nically successful interventions may reverse these patho- physiologic features in utero (Selamet Tierney et al., 2007), and such changes are more likely to yield a biventricular cir- culation at birth (Prosnitz et al., 2018). An additional consideration with regard to patient selec- tion for FAV is whether the LV is salvageable. In other words, will the LV be able to recover its function and effec- tively support the systemic circulation postnatally? In 2009, McElhinney et al. published revised criteria to ensure that the LV and mitral valve are not too hypoplastic, that is, z-score >−2, and that the LV is capable of generating adequate pressure (McElhinney et al., 2009). In 2018, Fried- man et al. updated these criteria to additionally evaluate the dimension of the ascending aorta and the mitral inflow time, the latter as a marker of diastolic dysfunction (Figure 1). The authors found that fetuses with LV pressure >47 mmHg and ascending aortic z-score >0.57 had a 92% chance of having a biventricular circulation following a technically successful intervention (Friedman et al., 2018). 3 | PROCEDURAL TECHNIQUE AND RESULTS One of the most important features of a technically success- ful FCI is the positioning of the fetus at the onset of the pro- cedure. In order to obtain access across the aortic valve for FIGURE 1 This diagram depicts the classification and regression tree analysis to predict fetal candidates that will have a biventricular (Biv) circulation at birth. AscAo = ascending aorta, MV = mitral valve, LV = left ventricle Adapted from Friedman et al., 2018. Improved technical success, postnatal outcome and refined predictors of outcome for fetal aortic valvuloplasty. Ultrasound in Obstetrics & Gynecology, 52(2), 212–220 2 CRYSTAL AND FREUD
- 3. balloon dilation, direct alignment needs to be visualized from the maternal abdomen through the fetal LV apex and across the outflow tract by ultrasound (Figure 2). Once the fetus has been adequately positioned, a small spinal needle is used for intramuscular delivery of paralysis and analgesia to the fetus. The angioplasty balloon/wire unit is prepared with the coronary wire through the balloon catheter with a Y-adapter attached to the end of the balloon. A coronary balloon/wire is used to accommodate the small size of the fetal aortic valve. After the needle introducer is opened, the balloon/ wire unit is advanced beyond the tip until it is fully exposed to allow unimpeded dilation. At this point, a marker is affixed to the balloon catheter. The balloon is drawn back into the needle and once fully covered, the distance between the needle hub and the marker on the catheter is noted. As such, the length of the needle is evident from landmarks external to the mother and fetus. An 18G or 19G needle introducer is placed into the mater- nal abdomen and advanced through the uterine wall until at the fetal thorax. Alignment is re-confirmed, and the introducer is passed through the fetal thorax and LV apex to the outflow tract. Once positioned, the stylet is removed, and the pre- prepared coronary balloon/wire unit is advanced to the tip of the needle based on the external markers. The coronary wire FIGURE 2 These line drawings depict the ideal alignment of the needle through the maternal abdomen to the fetus (left) and in the left ventricular outflow tract (right) Adapted from Tworetzky et al., 2004. Balloon dilation of severe aortic stenosis in the fetus. Circulation, 110, 2125–2131 FIGURE 3 Ultrasound images of (a) the needle traversing the maternal abdomen and fetal thorax to terminate in the left ventricle (LV), directed at the outflow tract; and (b) the balloon/wire unit advanced and positioned across the aortic valve (AV) for dilation Images courtesy of Boston Children's Hospital CRYSTAL AND FREUD 3
- 4. is advanced beyond the needle under direct ultrasound visuali- zation and maneuvered across the aortic valve into the ascend- ing aorta. The coronary balloon is subsequently advanced and positioned across the aortic valve until it is exposed according to the external marker on the catheter (Figure 3). The balloon is dilated to maximal inflation with a goal balloon: annulus ratio of 1.1–1.2 as reported previously (Marshall et al., 2005). Typically, several inflations are performed until ultrasound confirms either a broader jet of antegrade flow across the aortic valve or the presence of aortic regurgitation. Once the valvuloplasty has been performed, the entire coronary balloon/wire unit and needle are removed simulta- neously. Postprocedural monitoring is essential. Compli- cations include pericardial effusion/tamponade and/or bradycardia that may require acute intervention with pericar- diocentesis or administration of intracardiac epinephrine (Mizrahi-Arnaud et al., 2007). Technical success has been reported to range from 77 to 94% (Friedman et al., 2018; Galindo et al., 2017; Kovacevic et al., 2018), with higher success rates at centers with greater experience. Similarly, although fetal demise rates of ~10% were previously described (Freud et al., 2014; Kovacevic et al., 2018; Moon-Grady et al., 2015), a large center recently reported that their rate has decreased to <5% (Friedman et al., 2018). Importantly, no significant maternal complications have been reported (Wohlmuth, Tulzer, Arzt, Gitter, & Wertaschnigg, 2014). 4 | OUTCOMES Technically successful FAV may result in improved hemo- dynamics and size of left heart structures throughout the remainder of gestation, permitting a biventricular circulation at the time of birth (Figure 4). Of the first 100 patients to undergo FAV at a large center, Freud et al. reported that 38 of the 88 live-born patients were managed with a biven- tricular circulation from birth (43%). Importantly, after a median postnatal follow-up of 5.4 years, cardiac survival was better in the biventricular group as compared to the HLHS cohort (Figure 5) (Freud et al., 2014). In a report from the multicenter International Fetal Cardiac Intervention Reg- istry in 2015, 26% (23 of 90) of fetuses that did not undergo FAV were alive postnatally (22% with a biventricular circu- lation). In contrast, 80% (69 of 86) that underwent FAV were alive postnatally with 40% achieving a biventricular circulation (Moon-Grady et al., 2015). Most recently, improved survival at 10 years was noted among patients who underwent FAV in Europe (Kovacevic et al., 2018). FIGURE 4 (a) and (b) Fetal and neonatal echocardiograms of a patient with evolving hypoplastic left heart syndrome (HLHS) in utero who underwent a technically unsuccessful fetal aortic valvuloplasty; the left ventricle (LV) was inadequate at birth, and the patient was managed as HLHS. (c) and (d) Fetal and neonatal echocardiograms of a patient with evolving HLHS who had a technically successful intervention; the LV was able to support the circulation after birth, and the patient was managed as biventricular Adapted from Freud et al., 2014. Fetal aortic valvuloplasty for evolving hypoplastic left heart syndrome: Postnatal outcomes of the first 100 patients. Circulation, 130(8), 638–645 4 CRYSTAL AND FREUD
- 5. While this survival advantage seemed to be independent of the final circulation, the numbers were quite limited. The achievement of a biventricular circulation and improved survival are notable outcomes following FAV. However, such patients are not free from morbidity. In a series from a large center, nearly all patients with a biventri- cular circulation required postnatal intervention, which often consisted of aortic and mitral valve procedures. Valve replacements, in particular, were not uncommon with 39% requiring replacement of the aortic valve and 21% of the mitral valve (Freud et al., 2014). LV diastolic dysfunction and abnormal remodeling pose additional issues (Friedman et al., 2011, 2015). With regard to noncardiac outcomes, there has been no reported difference in somatic growth or neurodevelopmen- tal measures between patients managed as biventricular or HLHS (Freud et al., 2014; Laraja et al., 2017). Long-term follow-up of these patients is essential. 5 | BUILDING A TEAM The success of FCI requires the collaboration of an experi- enced, multidisciplinary team, including high-risk obstetrics, fetal and interventional cardiology, and anesthesia. Postna- tally, commitment to a biventricular strategy is also critical. At our center, we recently created a FCI team. We began by performing site visits to centers with experience and expertise and then proceeded with hands-on simulation in order to optimize communication and coordination. First, we developed inanimate molds to practice needle placement under ultrasound guidance. Subsequently, as initially reported by Kohl et al. in 2000 and more recently studied by Emery et al. in 2010, our team moved to an animal model to hasten our learning curve (Kohl, Strumper et al., 2000). In this envi- ronment with a fetal sheep, we were able to successfully per- form multiple procedures, including FAV, fetal pulmonary valvuloplasty, and atrial septal stent implantation. We believe this process will improve our workflow and ultimately lead to greater technical success. 6 | SUMMARY Fetal echocardiography allows for the early detection of con- genital heart defects that may progress in utero, such as severe, mid-gestation AS with evolving HLHS. Despite early struggles, technical success of FAV for this disease has improved, and a biventricular outcome with improved sur- vival may be achieved in select patients. Many challenges remain to determine the best candidates with salvageable LV's and to develop better technology to allow for greater, and perhaps earlier, procedural success. Critical evaluation of both local institutional practices in the process of FCI team building, as well as pooled long-term outcomes from multiple centers, is essential as this field evolves. ACKNOWLEDGMENTS None. ORCID Lindsay R. Freud https://orcid.org/0000-0002-1221-081X REFERENCES Allan, L. D., Sharland, G., & Tynan, M. J. (1989). The natural history of the hypoplastic left heart syndrome. International Journal of Cardiology, 25(3), 341–343 Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/2613383; http://www.sciencedirect.com/science/article/pii/016752738990226X Danford, D. A., & Cronican, P. (1992). Hypoplastic left heart syndrome: Pro- gression of left ventricular dilation and dysfunction to left ventricular hypo- plasia in utero. American Heart Journal, 123(6), 1712–1713 Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1595559; http://www.sciencedirect. com/science/article/pii/000287039290834I Emery, S. P., Kreutzer, J., McCaffrey, F. M., Sherman, F. S., Simhan, H. N., & Keller, B. B. (2010) The learning curve for a fetal cardiac intervention team. Minimally Invasive Surgery, 2010, 674185. Freud, L. R., McElhinney, D. B., Marshall, A. C., Marx, G. R., Friedman, K. G., del Nido, P. J., … Tworetzky, W. (2014). Fetal aortic valvuloplasty for evolving hypoplastic left heart syndrome: Postnatal outcomes of the first 100 patients. Circulation, 130(8), 638–645. https://doi.org/10.1161/ CIRCULATIONAHA.114.009032 Friedman, K. G., Freud, L., Escobar-Diaz, M., Banka, P., Emani, S., & Tworetzky, W. (2015). Left ventricular remodeling and function in children with biventricular circulation after fetal aortic valvuloplasty. Pediatric Cardi- ology, 36(7), 1502–1509. https://doi.org/10.1007/s00246-015-1193-6 Friedman, K. G., Margossian, R., Graham, D. A., Harrild, D. M., Emani, S. M., Wilkins-Haug, L. E., … Tworetzky, W. (2011). Postnatal left ventricular dia- stolic function after fetal aortic valvuloplasty. The American Journal of Car- diology, 108(4), 556–560. https://doi.org/10.1016/j.amjcard.2011.03.085 pii: S0002-9149(11)01418-4. Friedman, K. G., Sleeper, L. A., Freud, L. R., Marshall, A. C., Godfrey, M. E., Drogosz, M., … Tworetzky, W. (2018). Improved technical success, FIGURE 5 The Kaplan–Meier curve demonstrates better cardiac survival among patients managed with a biventricular circulation (BV) as opposed to the conventional univentricular strategy (HLHS) following fetal aortic valvuloplasty Adapted from Freud et al., 2014. Fetal aortic valvuloplasty for evolving hypoplastic left heart syndrome: Postnatal outcomes of the first 100 patients. Circulation, 130(8), 638–645 CRYSTAL AND FREUD 5
- 6. postnatal outcome and refined predictors of outcome for fetal aortic valvulo- plasty. Ultrasound in Obstetrics & Gynecology, 52(2), 212–220. https://doi. org/10.1002/uog.17530 Galindo, A., Gomez-Montes, E., Gomez, O., Bennasar, M., Crispi, F., Herraiz, I., … Martinez, J. M. (2017). Fetal aortic valvuloplasty: Experience and results of two tertiary centers in Spain. Fetal Diagnosis and Therapy, 42 (4), 262–270. https://doi.org/10.1159/000460247 Ghanayem, N. S., Allen, K. R., Tabbut, S., Atz, A. M., Clabby, M. L., Cooper, D. S., … Pediatric Heart Network Investigators. (2012). Interstage mortality after the Norwood procedure; results of the multi-center single ven- tricle reconstruction trial. The Journal of Thoracic and Cardiovascular Sur- gery, 144, 896–906. Kohl, T., Sharland, G., Allan, L. D., Gembruch, U., Chaoui, R., Lopes, L. M., … Silverman, N. H. (2000). World experience of percutaneous ultrasound- guided balloon valvuloplasty in human fetuses with severe aortic valve obstruction. The American Journal of Cardiology, 85(10), 1230–1233 pii: S0002-9149(00)00733-5. Kohl, T., Strumper, D., Witteler, R., Merschhoff, G., Alexiene, R., Callenbeck, C., … Scheld, H. H. (2000). Fetoscopic direct fetal cardiac access in sheep: An important experimental milestone along the route to human fetal cardiac inter- vention. Circulation, 102(14), 1602–1604 Retrieved from http://www.ncbi.nlm. nih.gov/pubmed/11015334; http://circ.ahajournals.org/content/102/14/1602. full.pdf Kovacevic, A., Ohman, A., Tulzer, G., Herberg, U., Dangel, J., Carvalho, J. S., … Fetal Working Group of the AEPC. (2018). Fetal hemodynamic response to aortic valvuloplasty and postnatal outcome: A European multicenter study. Ultrasound in Obstetrics & Gynecology, 52(2), 221–229. https://doi.org/10.1002/uog.18913 Laraja, K., Sadhwani, A., Tworetzky, W., Marshall, A. C., Gauvreau, K., Freud, L., … Newburger, J. W. (2017). Neurodevelopmental outcome in children after fetal cardiac intervention for aortic stenosis with evolving hypoplastic left heart syndrome. The Journal of Pediatrics, 184, 130–136 e134. https://doi.org/10.1016/j.jpeds.2017.01.034 Makikallio, K., McElhinney, D. B., Levine, J. C., Marx, G. R., Colan, S. D., Marshall, A. C., … Tworetzky, W. (2006). Fetal aortic valve stenosis and the evolution of hypoplastic left heart syndrome: Patient selection for fetal intervention. Circulation, 113(11), 1401–1405. Marshall, A. C., Tworetzky, W., Bergersen, L., McElhinney, D. B., Benson, C. B., Jennings, R. W., … Lock, J. E. (2005). Aortic valvuloplasty in the fetus: Technical characteristics of successful balloon dilation. The Journal of Pediatrics, 147(4), 535–539. pii:S0022-3476(05)00384-7. https:// doi.org/10.1016/j.jpeds.2005.04.055 Maxwell, D., Allan, L., & Tynan, M. J. (1991). Balloon dilatation of the aortic valve in the fetus: A report of two cases. British Heart Journal, 65(5), 256–258 Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/2039669; http://heart.bmj.com/content/65/5/256.full.pdf; http://heart.bmj.com/content/ heartjnl/65/5/256.full.pdf McCaffrey, F. M., & Sherman, F. S. (1997). Prenatal diagnosis of severe aortic stenosis. Pediatric Cardiology, 18(4), 276–281 Retrieved from http://www. ncbi.nlm.nih.gov/pubmed/9175524m; http://rd.springer.com/article/10.100 7%2Fs002469900174; http://download.springer.com/static/pdf/459/art%253 A10.1007%252Fs002469900174.pdf?originUrl=http%3A%2F%2Flink.springer. com%2Farticle%2F10.1007%2Fs002469900174&token2=exp=1450132544~acl= %2Fstatic%2Fpdf%2F459%2Fart%25253A10.1007%25252Fs002469900174.pdf% 3ForiginUrl%3Dhttp%253A%252F%252Flink.springer.com%252Farticle%252F10. 1007%252Fs002469900174*~hmac=a1c2f51b3dab5948659fcd024a76253a93e62 fcb864cdcdb34a57a0dc937c422 McElhinney, D. B., Marshall, A. C., Wilkins-Haug, L. E., Brown, D. W., Benson, C. B., Silva, V., … Tworetzky, W. (2009). Predictors of technical success and postnatal biventricular outcome after in utero aortic valvuloplasty for aortic stenosis with evolving hypoplastic left heart syndrome. Circulation, 120(15), 1482–1490. https://doi.org/10.1161/CIRCULATIONAHA.109. 848994 pii:CIRCULATIONAHA.109.848994. Mitchell, M. E., R, I., Gaynor, J. W., Wernosky, G., Nicolson, S., & Spray, T. L. (2006). Intermediate outcomes after the Fontan procedure in the current era. The Journal of Thoracic and Cardiovascular Surgery, 131, 172–180. Mizrahi-Arnaud, A., Tworetzky, W., Bulich, L. A., Wilkins-Haug, L. E., Marshall, A. C., Benson, C. B., … McElhinney, D. B. (2007). Pathophysiol- ogy, management, and outcomes of fetal hemodynamic instability during prenatal cardiac intervention. Pediatric Research, 62(3), 325–330. https:// doi.org/10.1203/PDR.0b013e318123fd3a Moon-Grady, A. J., Morris, S. A., Belfort, M., Chmait, R., Dangel, J., Devlieger, R., … Oepkes, D. (2015). International fetal cardiac intervention registry: A worldwide collaborative description and preliminary outcomes. Journal of the American College of Cardiology, 66(4), 388–399. Prosnitz, A. R., Drogosz, M., Marshall, A. C., Wilkins-Haug, L. E., Benson, C. B., Sleeper, L. A., … Friedman, K. G. (2018). Early hemodynamic changes after fetal aortic stenosis valvuloplasty predict biventricular circulation at birth. Pre- natal Diagnosis, 38(4), 286–292. https://doi.org/10.1002/pd.5232 Selamet Tierney, E. S., Wald, R. M., McElhinney, D. B., Marshall, A. C., Benson, C. B., Colan, S. D., … Tworetzky, W. (2007). Changes in left heart hemodynamics after technically successful in-utero aortic valvuloplasty. Ultrasound in Obstetrics & Gynecology, 30(5), 715–720. https://doi.org/10. 1002/uog.5132 Simpson, J. M., & Sharland, G. K. (1997). Natural history and outcome of aortic steno- sis diagnosed prenatally. Heart, 77(3), 205–210 Retrieved from http://www.ncbi. nlm.nih.gov/pubmed/9093035; http://heart.bmj.com/content/77/3/205.full.pdf Williams, I. A., Sleeper, L. A., Colan, S. D., Lu, M., Stephenson, E. A., Newburger, J. W., … Pediatric Heart Network Investigators. (2009). Func- tional state following the Fontan procedure. Cardiology in the Young, 19, 320–330. Wohlmuth, C., Tulzer, G., Arzt, W., Gitter, R., & Wertaschnigg, D. (2014). Maternal aspects of fetal cardiac intervention. Ultrasound in Obstetrics & Gynecology, 44(5), 532–537. https://doi.org/10.1002/uog.13438 How to cite this article: Crystal MA, Freud LR. Fetal aortic valvuloplasty to prevent progression to hypoplas- tic left heart syndrome in utero. Birth Defects Research. 2019;1–6. https://doi.org/10.1002/bdr2.1478 6 CRYSTAL AND FREUD