
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Femoro-acetabular impingement (FAI): Causes, classification, clinical features, tests, imaging and treatment
Similar to Femoro-acetabular impingement (FAI): Causes, classification, clinical features, tests, imaging and treatment (20)
More from Lokesh Sharoff
Recently uploaded
Recently uploaded (20)
Femoro-acetabular impingement (FAI): Causes, classification, clinical features, tests, imaging and treatment
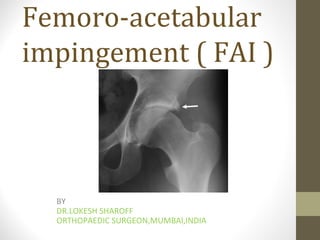
- 1. Femoro-acetabular impingement ( FAI ) BY DR.LOKESH SHAROFF ORTHOPAEDIC SURGEON,MUMBAI,INDIA
- 3. ABOUT There is reduced range of motion of hip due to uneven surfaces of the head of femur or acetabulum or both.
- 4. CAUSES 1> CONGENITAL increased retroversion 2> ACQUIRED -post traumatic -- #neck femur -following femoral osteotomy -perthes disease -scfe
- 5. CLASSIFICATION GANZ ET AL 3 TYPES 1> cam 2> spincer 3> mixed
- 6. CAM TYPE --refers to an abnormal bony bump at the head neck junction of the femur . --This nonspherical portion is usually found anterosuperiorly . --This abnormal ‘bump’ or insufficient concavity of the femoral head-neck junction decreases femoral head-neck offset and causes impingement on the acetabular labrum and articular cartilage with daily activities.
- 7. CAM PATHOPHYSIOLOGY • Cartilage is affected delamination of articular cartilage then labrum is displaced outwards and superiorly.
- 8. PINCER TYPE Pincer impingement is an acetabular sided morphologic abnormality characterized by over coverage of the femoral head The femoral head makes contact with the acetabulum due to overcoverage
- 9. Pincer pathophysiology Unlike cam type ,labral lesions occurs before the cartilage lesions labrum is crushed causing intrasubstance tears and sometimes para labral cysts. With time , articular cartilage is also damaged. Healing of labrum forms an ossified rim which further worsens the acetabular coverage.
- 10. PINCER SUBDIVISION FOCAL – due to retroversion GLOBAL – due to protruso acetabuli
- 11. CLINICAL FEATURES -- active young adult (atheletes and ballet dancers) -- slow growing groin pain -- increased by prolonged walking or sitting -- can be referred to the knee --GAIT – antalgic --ROM – flexion and internal rotation will be restricted
- 12. TESTS -- ANTERIOR IMPINGEMENT TEST -- POSTERIOR IMPINGEMENT TEST
- 13. IMAGING
- 14. IMAGING ACETABULAR RETROVERSION ( FOR PINCER LESIONS) 1> CROSS OVER SIGN – MILD MODERATE SEVERE 2>POSTERIOR WALL SIGN
- 16. The posterior wall sign: Normally the center of the femoral head lies medial to the posterior wall. When it lies lateral to the posterior wall, the posterior wall sign is said to be positive and implies a retroverted acetabulum. The sign also reflects how much posterior wall coverage exists
- 18. IMAGING FOR CAM LESIONS --cross leg lateral view ,-- dunn view ,--modified dunn view 1– circle is drawn over femoral head which shows a smooth contour .any lesion outside is a cam lesion. 2—ALPHA ANGLE – normal 42 , if > 50.5 diagnostic of a cam lesion
- 21. CT SCAN / MRI CT SCAN – 3D CT helps to identify exact size and location of patholgy that helps in surgery MRI SCAN – helps to find out soft tissue lesions like labral tears , paralabral cysts, articular cartilage defects , cartilage delamination, ossification of acetabular rim and loss of sphericity of femoral head due to fibrocystic changes .
- 22. NON SURGICAL MANAGEMENT --initial trial of conservative management includes restriction of atheletic activities and Nsaids . But sx rx is usually unsuccessful and operative rx is preferred early.
- 23. Surgical treatment INDICATIONS – -- joint space narrowing of 1-2mm -- extent of damage to acetabular labral chondral complex --severe acetabular retroversion --femoral head asymmetry --high riding GT in cam impingement
- 24. SURGERIES 1– SURGICAL DISLOCATION AND TRIMMING OF CAM AND PINCER LESIONS 2– CORRECTION BY ARTHROSCOPY 3– PERIACETABULAR OSTEOTOMY FOR FOCAL OVERCOVERAGE 4– TOTAL HIP REPLACEMENT
- 25. SURGICAL DISLOCATION OF HIP INDICATIONS – -- cam type lesion -- pincer type lesion cam type lesion with 1mm of joint space reduction as this approach would allow conversion to arthroplasty if needed.
- 26. ARTHROSCOPY INDICATIONS --Cam type lesion without proximal femoral deformity. --isolated acetabular retroversion with or without cam type deformity
- 27. LIMITATIONS OF ARTHROSCOPY -- steep learning curve -- injury to neuro-vascular structures from the entry portals -- incomplete removal or -- excessive removal of bone at the cam lesion leading to a fracture
- 28. ARTHROSCOPY CONSISTS OF 2 COMPONENTS 1– CENTRAL COMPARTMENT – which consists of labrum and all parts medial to it 2– PERIPHERAL COMPARTMENT – which consists of parts lateral to labrum but within the capsule and includes the head neck junction
- 29. PERIACETABULAR OSTEOTOMY INDICATIONS – --acetabular retroversion with an associated posterior wall sign (cartilage in the antero-superior area must be intact)
- 30. THANK YOU