VIP Call Girl Sector 88 Gurgaon Delhi Just Call Me 9899900591
Primary neurectoermal tumor of kidney
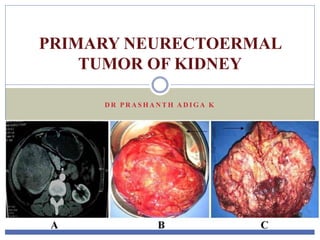
1. D R P R A S H A N T H A D I G A K
PRIMARY NEURECTOERMAL
TUMOR OF KIDNEY
2. INTRODUCTION
Primitive neuroectodermal tumors (PNET) are a group of
small round cell malignancies with neural crest origin.
They are highly aggressive and rare.
These tumors may originate in the central nervous system
or in other tissues peripherally.
The peripheral type is seen typically in the soft tissues of
the chest wall and paraspinal region and unusually along
the genitourinary tract
3. INTRODUCTION
PNET rarely presents as an organ-derived neoplasm.
The overall incidence of peripheral PNET is 1% of all
sarcomas.
The incidence of PNET in the abdomen and pelvis,
including the retroperitoneum, is about 14% of all
peripheral PNETs.
Renal PNET is extremely rare with fewer than 50 cases in
the literature
4. INTRODUCTION
EWS/PNET occurs rarely as a primary renal neoplasm
and exhibits highly aggressive biological behavior.
Most patients are young adults with a median age of 28
years (range 4 to 69) and a slight male predominance
(1.5:1).
Because of their morphological resemblance to
neuroblastomas, they have been considered to be neural
crest derivatives
5. FACTS
Until now, the largest series of rPNET was published
by Yuvaraja B and al. This series included 16 patients
who were treated in Tata Memorial Hospital in India
6. ORIGIN
The origin of this tumor is unknown, but it seems that
it derives from cells that migrated from the neural
tube, with variable capability of ectodermal or
neuronal differentiation.
7. SIGNS AND SYMPTOMS
The presenting symptoms and images of rPNET are non-
specific and similar to other renal tumors.
Therefore it is often difficult to distinguish rPNET from
renal cell carcinoma and Wilm’s tumor.
The clinical symptoms and signs are nonspecific,
comprising flank or abdominal pain, palpable mass and
hematuria in decreasing order.
8. SIGNS AND SYMPTOMS
rPNET appears to be an unique clinical entity that behaves
more aggressively than PNET arising at other sites.
Approximately 20% to 50% of patients present with
distant metastases, most commonly to regional lymph
nodes, bone, bone marrow, lung, and liver.
The 5-year disease-free survival rate of rPNET is about
45% to 55%
9. Lab findings
Laboratory findings are mostly unremarkable but
increased lactate dehydrogenase is sometimes reported.
10. RADIOLOGY
Radiographic features of PNETs are large size, lack of
extensive parenchyma infiltration, lack of renal vein
invasion, diffuse large calcification, areas of internal
hemorrhage and necrosis, and peripheral hypervascularity
11.
12.
13.
14. Histological examination
A small rounded cell tumor with hyperchromatic nucleus
and scant cytoplasm in a fibrotic stroma.
Immunohistochemical finding was compatible with PNET
or Ewing’s sarcoma (positive for neuron specific enolase
(NSE), vimentin, CD99 and negative for desmin,
leukocyte common antigen (LCA) and chromogranin)
15. D/D
Carefully selected immunohistochemical panel is
important for differentiating this tumor from other small
round cell tumors of the kidney such as
Rhabdomyosarcoma,
Neuroblastoma,
Clear cell sarcoma of the kidney,
Desmoplastic small round cell tumor (DSRCT),
Carcinoid tumor,
Nephroblastoma
Ewing’s sarcoma
16. IMMUNOHISTOCHEMISTRY
Immunohistochemically, PNET cells express vimentin,
NSE and CD99.
The positive reactivity to CD99 is a clue for PNET
diagnosis.
MIC2 gene product (a monoclonal antibody that
recognizes the glycoprotein p30/32 MIC2) which has
fairly recently been introduced, is reported to show
immunoreactivity in 90%-95% of Ewing’s sarcoma and
PNET
17. IMMUNOHISTOCHEMISTRY
The cloning of the breakpoints of the specific
chromosomal translocations t (11; 22)(q24; q12) and t
(21; 22)(q22; q12) that are present in approximately
90% of PNET/Ewing’s sarcomas permits the use of the
reverse transcription polymerase chain reaction (RT-
PCR) for the detection of specific fusion transcripts in
these tumors.
21. The part of tumor cells showed positive expression of NSE.
22. PATHOLOGY
The diagnosis of rPNET mainly depends on pathologic
characteristics and biomarkers.
rPNET is characterized by small uniform round cells with
dark nuclei, illdefined cytoplasmic borders, and poorly-
formed rosettelike structures.
Additionally, CD99 also named MIC-2 antigen is crucial
in the diagnosis of rPNET and the positive expression of
CD99 has been demonstrated in more than 90% of rPNET
23. PATHOLOGY
CD99 is not specific and cannot be used as an absolute
biomarker.
Cytogenetic analyses may therefore be helpful in the
diagnosis of rPENT.
The translocation of t(11:22) (q24:q12) with the fusion
transcript between the EWS gene (22q12) and the ETS-
related oncogene (11q24) have been detected in more than
90% of patients
25. WILMS TUMOR
• The features favoring the diagnosis of blastemal Wilms
tumor are young age and positivity of blastemal elements
for vimentin, low molecular weight cytokeratin, epithelial
membrane antigen, and WT1.
• Immunohistochemistry is very useful to differentiate it
from renal primitive neuroectodermal tumor/EWING
tumor because neuroblastomas are consistently positive
for NSE and chromogranin and mostly negative for
CD99.
26.
27. TREATMENT
Surgical excision remains the most important modality of
management which has shown the survival advantage.
Despite aggressive treatment of these tumors by
combination therapy with surgery, chemotherapy, and
radiotherapy, the prognosis remains poor and overall 5-
year survival rates have been reported at 45% to 55%.
28. TREATMENT
Before the routine use of adjuvant chemotherapy, the 5-
year survival rate in patients with rPNET was less than
10%.
Cyclophosphamide (C), actinomycin (A), and vincristine
(V) were found to be effective in this group of diseases.
Later, it was demonstrated that doxorubicin (D) was also
an active agent.
29. TREATMENT
The most recent additions to the list of active agents in
this disease have been ifosfamide (I)and etoposide (E).
The addition of latter 2 drugs to the previous standard
treatment of VAC alternating with VCD has been shown
to improve the overall and disease-free survival in patients
with nonmetastatic skeletal Ewing’s sarcoma
30. TREATMENT
The use of dose-intensive combination regimen lasting
about 49 weeks is the std.
At TMH institution they have used these 6 drugs in EFT-
2001 protocol.
Because of the high incidence of febrile neutropenia, all
patients receive prophylactic granulocyte-colony
stimulating factor (G-CSF) after courses.
33. RADIATION
Radiation therapy is useful in treating these patients,
especially when the resection is not possible or residual
disease is present.
It is logical to give radiotherapy in the presence of
Gerota’s fascia involvement and positive surgical margins.
Radiation dose varied from 5040 to 6000 rads
34. TREATMENT
Thomas et al.24 and Karnes et al.25 have described a case
of PNET kidney associated with IVC thrombus which was
removed at the time of nephrectomy
35. Radical nephrectomy was immediately done based on the findings of CT of the right
kidney.
rPENT who immediately underwent six cycles of chemotherapy with ifosfamide,
etoposide, and adriamycin.
36. KEY POINTS
The preferred treatment for rPENT is surgical resection
associated with chemotherapy and radiotherapy treatment.
The role of radiotherapy is not clear, but it may be
advocated in locally advanced disease and involvement of
Gerota’s fascia.
Most cases of rPNET may recur after nephrectomy
without adjuvant chemotherapy.
37. CONCLUSIONS
PNET are small round cell tumors of presumed neural
crest origin arising outside the central and sympathetic
nervous system.
PNET of the kidney is a distinct clinical entity with
aggressive behavior.
The tumor diagnosis is based on a classical histologic and
IHC features complemented by cytogenetics and
molecular analysis.
38. CONCLUSIONS
Aggressive multimodality treatment is recommended to
manage these tumors.
Complete resection of the kidney with node dissection
should be performed if at all feasible.
The best results are seen with combination chemotherapy
that is used for other round cell tumors like Ewing’s
sarcoma
The role of radiotherapy is not clear but may be advocated
in locally advanced disease and involvement of Gerota’s
fascia