
Recommended
Recommended
More Related Content
Similar to not all beta blockers are same powerpoint.pptx
Similar to not all beta blockers are same powerpoint.pptx (20)
Recently uploaded
Recently uploaded (20)
not all beta blockers are same powerpoint.pptx
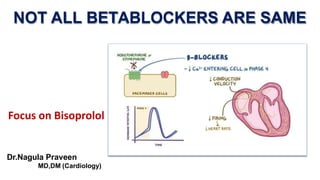
- 1. NOT ALL BETABLOCKERS ARE SAME Focus on Bisoprolol Dr.Nagula Praveen MD,DM (Cardiology)
- 2. Beta Blockers • Beta-blockers refer to a mixed group of drugs with diverse pharmacodynamics and pharmacokinetic properties. • They have shown long term beneficial effects on mortality and cardiovascular disease (CVD) when used in people with heart failure or acute myocardial infarction. • Beta-blockers were thought to have similar beneficial effects when used as first-line therapy for hypertension. Farzam K et al., Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available
- 3. Classification Of β Blockers JAPI Suppl; Dec 2009; 57: 7 – 12
- 4. Am J Cardiol 2010;106:1819 –1825 There are valid reasons to question the utility of certain beta blockers in treating hypertension. Many of the perceptions about beta blockers are derived from data obtained from studies of traditional agents or combinations of diuretics and blockers. There are intrinsic differences among beta blocker class. The vasodilatory beta blockers, which have generally not been included in comparative meta-analyses, lower blood pressure to a similar degree as other antihypertensive drugs, may provide better central aortic pressure reductions than traditional blockers, and are associated with neutral or favorable metabolic effects. lies not in global When addressing the question of beta blockers’ effectiveness, the answer generalizations but in assessing individual patients and specific beta blocking agents.
- 5. For the ischemic patient, be it early or late intervention post-myocardial infarction, or chronic ischemia in non-surgical and surgical patients, the significant benefits from beta-blockers in reducing cardiovascular end-points stem from beta-1 blockade. Likewise for the heart failure patient, on a background of ACE-inhibition, beta-1 blockade (the common property of carvedilol, metoprolol and bisoprolol) is responsible for the 35% reduction in all-cause mortality. Central obesity in younger subjects is linked to endothelial inflammation and dysfunction, insulin resistance, markedly increased sympathetic nerve activity and increased cardiac output, heart rate and blood pressure - hemodynamic scenario ideal for beta-1 blockade International Journal of Cardiology 120 (2007) 10–27
- 6. In younger hypertensives beta-blockers reverse both ECG – and echocardiographic – LVH. High beta-1 selectivity ensures reversibility of echocardiographic LVH at least as great as the action of ACE-inhibitors. Beta-blocker-induced metabolic disturbance (lipids, blood sugar and insulin-resistance) stems from beta-2 blockade (and possibly beta-3 blockade). Such disturbances are avoided by high beta-1 selectivity, beta-2/3 intrinsic sympathomimetic activity or alpha blockade. In trials involving younger/middle-aged overweight hypertensives (MRC mild Hypertension, IPPPSH, MAPHY, UKPDS), with relatively narrow pulse pressures, first-line beta-blockade has been more effective than placebo and diuretics, and at least as good as ACE-inhibitors, in preventing coronary events International Journal of Cardiology 120 (2007) 10–27
- 7. Elderly systolic hypertensives tend to have low plasma renin activity, insensitive beta- receptors, low/normal cardiac output and non-compliant arteries (wide pulse pressure). Such a haemodynamic scenario is unsuited to certain first-line beta-blockers e.g. atenolol and propranolol. First-line low-dose diuretic therapy with second-line beta-blocker therapy, has a track record at least as good as other combination therapies in reducing cardiovascular events in the elderly hypertensive, with the added bonus of a 30% reduction in the risk of bone fractures. Overweight/obesity in the younger/middle-aged hypertensive, and its accompanying increased sympathetic nerve activity, is a positive indication for beta-1 blockade and not a relative contra-indication. International Journal of Cardiology 120 (2007) 10–27
- 8. 2017 The Role of Beta-blockers in Hypertension Adv Exp Med Biol. 2017;956:149-166. β-blockers for Hypertension: Are they Going Out of Style?
- 9. β-blockers (BB) in HF treatment
- 10. BB reduce mortality and morbidity in symptomatic patients with HFrEF, despite treatment with an ACEI and, in most cases, a diuretic, but have not been tested in congested or decompensated patients. There is consensus that BB and ACEIs are complementary, and can be started together as soon as the diagnosis of HFrEF is made. There is no evidence favouring the initiation of treatment with a BB an ACEI has been started. BB should be initiated in clinically stable patients at a low dose and gradually up-titrated to the maximum tolerated dose. In patients admitted due to acute HF (AHF) BB should be cautiously initiated in hospital, once the patient is stabilized. Beta-blockers are recommended in patients with a history of myocardial infarction and asymptomatic LV systolic dysfunction to reduce the risk of death European Heart Journal (2016) 37, 2129– β-blockers (BB) in HF treatment
- 11. 300:1 increasing ß1 -selectivity increasing ß 2-selectivity ICI 1.8:1 Propranolol Bisoprolol 1:75 Atenolol Betaxolol no selectivity Ratio of constants of inhibition Metoprolol 1:35 1:35 1:20 Wellstein A et al. J Cardiovasc Pharmacol 1986; 8 (Suppl. 11): 36-40 Wellstein A et al. Eur Heart J 1987; 8 (Suppl. M): 3–8 ß1-selectivity of Various ß-blockers
- 12. Bisoprolol Bisoprolol is a cardioselective β1-blocker. It is used along with other β 1-blockers to treat multiple heart diseases such as congestive heart failure, without having the unwanted effect of the β2 receptor blocking, which can affect multiple systems in the body. Bisoprolol is considered to be one of the selective agents indicated in the treatment plan of compensated heart failure, along with carvedilol and metoprolol. Selective β - blockers are considered the first-line treatment for chronic stable angina. It is also FDA approved for the treatment of hypertension, post, or recent myocardial infarction (MI). Bazroon AA et al., Treasure Island (FL): StatPearls Publishing; 2021 Jan-.
- 13. Heart Kidney Heart Rate Force of Contraction Secretion of Renin Beta 1 ↑ CO ↑ PR ↑ BP ↑ Work Load on Heart Heart Failure, LVH Bisoprolol Mechanism of Action: Bisoprolol
- 14. *dose-dependent Criteria Bisoprolol Atenolol Metoprolol Acebutolol Celiprolol Plasma elimination half-life (h) 10 – 12 6 – 9 3 – 4 7 – 13 5 Absorption (%) > 90 50 > 95 70 50 First-pass effect – – + + – Bioavailability (%) 88 50 50 40 – 60 50* Protein binding (%) 30 3 12 11 – 25 25 Active metabolites – – – + – Balanced clearance + – – – – Borchard U. ß-Rezeptorenblocker, Klinik und Praxis, Aesopus Verlag 1996 Why Bisoprolol??
- 15. –16.5 –12.4 –14.2 –9.9 –12.2 –10.9 –13.2 –8.9 p = 0.03 0 –5 –10 –15 –20 day (6 a.m. – 10 p.m.) (6 a.m. – noon) night (10 p.m. – 6 a.m.) last 4 hours of dosing interval (6 a.m. – 10 a.m.) p = 0.03 p = 0.54 p <0.05 mean change in systolic blood pressure (mm Hg Bisoprolol Atenolol ( n = 107) ( n = 96) S ± SEM BISOPROLOL Vs ATENOLOL Neutel JM et al. Am J Med 1993; 94:181–187 ABPM technique were used to compare between the bisoprolol (10 to 20 mg OD) and atenolol (50 to 100 mg) for blood pressure reduction n=203
- 16. p<0.001 p<0.01 0 –2 –4 –6 –8 –10 –12 –14 –16 –12.8 –8.9 –11.5 –7.7 –9.6 –8.5 –10.9 –7.3 p=0.41 p<0.01 mean change in diastolic blood pressure (mm Hg ) day (6 a.m. – 10 p.m.) (6 a.m. – noon) night (10 p.m. – 6 a.m.) last 4 hours of dosing interval (6 a.m. – 10 a.m.) (n = 96) (n = 107) Bisoprolol Atenolol S ± SEM Neutel JM et al. Am J Med 1993; 94:181–187 BISOPROLOL Vs ATENOLOL
- 17. Haasis R et al. Eur Heart J 1987; 8 (Suppl M): 103–113 40 20 0 60 80 100 90% SBP 66% HR 93% 54% RPP 92% 60% % Bisoprolol: 24 H Efficacy In Comparison To Metoprolol (BISOMET Study) The effects of the beta blockers on systolic blood pressure, heart rate and rate-pressure product during exercise, 24 h and 3h at rest after administration (p.a.) were compared with the values obtained in the baseline exercise test (El) n = 87 Bisoprolol 10 mg Metoprolol Under Exercise Conditions
- 18. mm Hg 180 160 140 120 100 80 90 80 70 60 50 SBP n.s. DBP 2-4 weeks 0 + 2 + 4 weeks placebo ß-blocker ** p < 0.01 *p < 0.05 n.s.= not significant HR beats/min Bisoprolol (n = 44) Metoprolol (n = 43) * ** ** * ** BISOMET Study Haasis R et al. Eur Heart J 1987; 8 (Suppl M): 103–113 At rest
- 19. Comparison of Bisoprolol to a metoprolol for control heart rate and blood pressure in mild to moderate hypertensive patients (CREATIVE Study) Bisoprolol provided superior dynamic HR reduction and non-inferior dynamic BP reduction vs. metoprolol . No new safety concerns were found. n=186 Treatment duration: 12 weeks Hypertens Res. 2017 Jan;40(1):79-86
- 20. Comparing Beta-Blocking Effects of Bisoprolol, Carvedilol and Nebivolol • Beta-blocking effi cacy of bisoprolol, carvedilol and nebivolol both at rest and during exercise. In addition, we also determined potential effects of beta-blockade on quality of life (QOL). Hemodynamic Effects -Compared to baseline, heart rate during exercise was decreased at 3hr by bisoprolol (–24%), carvedilol (–17%) and nebivolol (–15%) - At the end of 1 week of chronic administration by bisoprolol (–14%), carvedilol (12 h!; –15%) and nebivolol (–13%) Quality of Life Total QOL with carvedilol was slightly but significantly lower than that with placebo, nebivolol and bisoprolol in all cases. Cardiology 2006;106:199–206
- 21. CIBIS II – Cardiac Insufficiency Bisoprolol Study • Double-blind, placebo-controlled, randomised trial • 2,647 patients included (NYHA III + IV) • Bisoprolol administered on top of standard therapy (diuretic + ACE inhibitor) • Study Objective • Primary objective • All-cause mortality Lancet. 1999 Jan 2;353(9146):9-13. • Secondary objectives Cardiovascular mortality Hospital admissions Cardiovascular mortality or cardiovascular hospital admissions Permanent treatment withdrawal
- 22. Survival 34% reduction in all-cause mortality with bisoprolol 1.0 0.8 0.6 0 0 200 600 800 400 Time after inclusion (days) Survival Bisoprolol: 156 deaths (n = 1327) Placebo: 228 deaths (n = 1320) log rank test, p < 0.0001 Lancet. 1999 Jan 2;353(9146):9-13.
- 23. Analysis of time to death Sudden death Pump failure Myocardial infarction Other cardio- vascular deaths Non-cardio- vascular deaths Unknown cause of death Hazardratio: 0.56 0.74 0.85 1.17 0.75 0.45 (95% CI) (0.39 – 0.80) (0.48 – 1.14) (0.31 – 2.34) (0.67 – 2.03) (0.37 – 1.50) (0.27 – 0.74) 83 6% 48 4% 36 3% p=0.17 p=0.75 p=0.58 p=0.41 p=0.0012 Bisoprolol (n = 1327) Placebo (n = 1320) Patients 100 p=0.0011 0 20 40 60 80 47 4% 7 1% 8 1% 28 2% 23 2% 14 1% 18 1% 23 2% 49 4% Lancet. 1999 Jan 2;353(9146):9-13.
- 24. Main results at a glance • All-cause mortality (independent of aetiology) by 34% (p<0.0001) • Sudden death by 44% (p<0.0011) • All-cause hospital admissions by 20% (p<0.0006) • Hospital admissions due to worsening heart failure by 36% (p<0.0001) In the bisoprolol-treated group of patients there was a reduction in Lancet. 1999 Jan 2;353(9146):9-13.
- 25. Study Conclusions • CIBIS II successfully demonstrated that ß1-selective bisoprolol given in addition to standard therapy – • Reduces significantly all-cause mortality and • All-cause hospitalisation in CHF patients • Bisoprolol is the first ß-blocker which has proven its efficacy in a single large-scale CHF study with all- cause mortality as primary objective • Bisoprolol was as well tolerated as placebo with a permanent treatment withdrawal rate of 15% in both groups Lancet. 1999 Jan 2;353(9146):9-13.
- 26. Monotherapy with beta-blocker bisoprolol (first 6 mos) 10mg O.D. n=505 Primary Endpoint: Time-to-the-first-event of combined all-cause mortality and all-cause hospitalization throughout study. Secondary Endpoint: Combined primary endpoint at end of monotherapy phase; individual components of primary endpoint at study end and at end of monotherapy phase. CIBIS III Trial Monotherapy with ACE-inhibitor enalapril (first 6 mos) 10mg B.I.D. n=505 1010 patients > 65 years with mild to moderate CHF (NYHA class II or III) and LV ejection fraction < 35% in 3 months prior to randomization, clinically stable CHF for 7 days Randomized 32% female, mean age 72 years, mean follow-up 1.22 years 13% received aldosterone-receptor blocker and 84% diuretic Combination beta-blocker and ACE-inhibitor therapy (6-24 mos) Circulation. 2005 Oct 18;112(16):2426-35.
- 27. CIBIS III Trial Summary • Among patients with newly diagnosed mild to moderate heart failure, a strategy of initial treatment with the beta-blocker bisoprolol did not meet the criteria for non-inferiority in the per-protocol population for death or hospitalization compared with a strategy of initial treatment with the ACE-inhibitor enalapril. • Non-inferiority was met in the intent-to-treat population. • Current guidelines recommend first-line therapy with an ACE-inhibitor after initial heart failure diagnosis, followed by addition of beta-blocker. Presented at ESC 2005 Circulation. 2005 Oct 18;112(16):2426-35.
- 28. Outcomes of major randomized, placebo-controlled trials in patients with heart failure and reduced ejection fraction Am J Cardiovasc Drugs (2017) 17:361–373
- 29. Journal of Internal Medicine, 2014, 275; 134–143
- 30. Design and results of the main clinical trials of beta-blockers in heart failure CV, cardiovascular; HF, heart failure; LVEF, left ventricular ejection fraction; NNT, number needed to treat; NS, not significant; NYHA, New York Heart Association. All studies analyzed beta-blockers vs placebo, except COMET (carvedilol vs metoprolol tartrate). All risk reductions are significant, unless otherwise indicated. * LVEF was not an inclusion criterion, but 36% of patients had a LVEF > 35%; the patients included were older than 70 years of age. Rev Esp Cardiol. 2019;72(10):844–852
- 31. Clinical Pearls Essential hypertension • Meta analysis has shown that Atenolol does NOT reduce cardiovascular mortality and morbidity or MI in patients with uncomplicated HTN (n=17671) • In another meta analysis (n=105951), β blockers when compared to other antihypertensive agents do not reduce MI or mortality and have shown ↑ risk of stroke in elderly (> 60 yrs) by 16% • β blockers reduce risk of MI and mortality in patients with essential HTN with ACS, post MI with symptomatic/ asymptomatic LV dysfunction Heart failure • Bisoprolol, metaprolol (SR) and carvedilol all have been shown to - reduce symptoms of HF -↑ QOL scores in HF - ↓ risk of death (RRR 30%) -combined risk of hospitalizations (RRR 40%) death and
- 33. Summary All beta blockers are majorly approved for the treatment of heart failure and hypertension. They produce unique nitric oxide–mediated vasodilatory effects, lacks intrinsic sympathomimetic activity, and possess a tolerability profile. For heart attack survivors, people with angina, or those with heart failure, beta blockers are a must-use medication because they have been proven to help prevent stroke and other cardiovascular problems. β‐Blockers have improved survival and are one of the cornerstones in the treatment of ischemic heart disease; they exert an antianginal effect by reducing the myocardial workload and oxygen demand. The effects of β‐blockers have been extensively investigated in patients with AMI and the current practice guidelines also recommend the use of β‐blockers in all patients after AMI unless contraindicated