
Recommended
More Related Content
What's hot
Similar to Skin Anatomy Guide
Similar to Skin Anatomy Guide (20)
Recently uploaded
Recently uploaded (20)
Skin Anatomy Guide
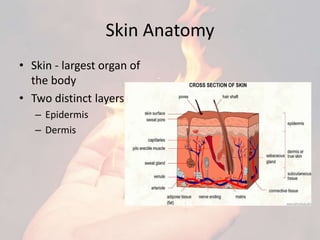
- 1. Skin Anatomy • Skin - largest organ of the body • Two distinct layers : – Epidermis – Dermis
- 2. Classification of burn injury
- 4. Electrical Burn • Signs and symptoms of an electrical burn may vary according to the type , intensity of current and area of the body the electric current passes. • Contact sites – – first contact with electricity – where patient was grounded • Wound at initial contact – charred and depressed , skin appears yellow and ischaemic . • Ground site – appears as explosion out of the tissue at the site, dry in appearance.
- 5. • Consequences : – Necrosis – Blood supply to surrounding tissue and muscle may be altered – Cardiac difficulties : arrhythmias, ventricular fibrillation. – Respiratory arrest – Renal failure – excessive protein breakdown and shock – Acute spinal cord damage , vertebral fracture.
- 7. Extent of burned area
- 8. Complications of burn injury Infection Pulmonary complications Metabolic complications Cardiovascular complications Heterotopic ossification Neuropathy Pathological scars
- 9. Dermal healing • Inflammatory phase • Proliferative phase • Maturation phase Epidermal healing Burn wound healing
- 10. Epidermal healing • Burn injures just the epidermis. • Stimulus for epithelial growth – presence of an open wound exposing subepithelial tissue to environment. • Intact epithelium covers an exposed wound through mitosis and ameboid movements. • Epithelial cells stop migration from when they are completely in contact with other epithelial cells. (contact inhibition). • After this, cells begin to form various layers of epithelium. • Adequate nutrition and blood supply to be provided for continuous migration and proliferation or else new cells die.
- 11. • This process most evident in partial thickness burns that has intact hair follicles and glands. • Cells migrate outwardly from appendages (epidermal islands) • Damage to sebaceous glands cause dryness and itching of healing wound. • Skin may split . • To teach lubrication and moisturizing cream application to newly healed tissues.
- 12. Dermal healing
- 13. • Tissue deeper than epidermis, dermal healing or scar formation occurs. • Scar formation is divided into 3 phases : – Inflammatory – Proliferative – Maturation
- 14. Medical management of Burns • Initial management : – Establish and maintain an airway. – Prevent cyanosis, shock and hemorrhage. – Establish baseline data on the patient, such as extent and depth of burn injury. – Prevent or reduce fluid loses. – Clean the patient and the wounds. – Examine injuries. – Prevent pulmonary and cardiac complications.
- 15. • Hydrotherapy tanks or whirlpool tubs have some disinfectant in water to assist in infection control. • Water temperature should be 37o -40oC. • Adherent dressing removed. • Converted to showers, spraying or bed baths.
- 16. • Technique for applying topical cream or ointment. – Open technique. – Closed technique. • Closed technique consists of several layers: – First layer is nonadherent. – Followed by cotton padding. – Final layer consists of roll gauze or elastic bandages.
- 18. Surgical management of wound burn • Primary excision – surgical removal of eschar. • Patient taken to surgery within 1 week of injury. • Burns wound closed with grafts. • Types of grafts : – Autograft – Allograft – Xenograft • Advanced technique foe burns wound care is Skin substitutes. Types of skin substitutes: 1. Cultured epidermal autografts (CEA) 2. Cultured autologous composite grafts 3. Allergic skin substitue 4. Cultured dermis (temporary) 5. Cultured dermis (definitive)
- 19. Skin grafting procedure • Donor site. • Wounds heal by re-epithelialization . • Thinner skin graft – better adherence; thicker skin graft – better cosmetic result. • Sheet graft and mesh graft . • Successful adherence – sufficient vascularity within wound bed. • Survival of skin graft depends on several factors: – Circulation, nutritive supply to grafts. – Inosculation. – Penetration of host vessels into graft site.
- 21. Surgical correction of scar contracture • If PT interventions are unsuccessful in averting scar contracture formation, and limitation noted in ROM and function, surgery may be required. • Z- plasty, serves to lengthen a scar by interposing normal tissue in the line of the scar. • Skin grafts used for more severe contractures.
- 23. Physical therapy management • Goals of physiotherapy treatment: – Wound and soft tissue healing is enhanced. – Risk of infection and complications is reduced. – Risk of secondary impairments is reduced. – Maximal ROM is achieved. – Pre- injury level of cardiovascular endurance is restored. – Good to normal strength is achieved. – Independent ambulation is achieved. – Independent function in BADL and IADL is increased. – Scar formation is minimized. – Patient, family, caregivers understanding of expectations and goals and outcomes is increased. – Aerobic capacity is increased. – Self- management of symptoms is improved.
- 24. Positioning and splinting • Started on day of admission. • Outcomes of positioning : 1. Minimize edema. 2. Prevent tissue damage. 3. Maintains soft tissue in an elongated state. • Splinting can be viewed as an extension of the positioning program. • Indications for use of splints: 1. Prevention of contractures. 2. Maintenance of ROM achieved during an exercise session or surgical release. 3. Correction of contractures. 4. Protection of a joint or tendon. • Types of splints : • Static • Dynamic
- 29. Active and passive exercises
- 30. Resistive and conditioning exercise • Burns patient lose body weight and lean muscle mass. • Exercises consist of isokinetic, isotonic or other resistive training devices. • Vitals to be monitored. • Patients to be encouraged to participate in exercises that stresses cardiovascular function like walking, cycle ergometry, treadmill walking, staircase climbing etc.
- 31. Ambulation • Initiated at earliest appropriate time. • Ambulation initiated after skin graft, lower extremities should be wrapped in elastic bandages (fig of 8) to support new skin grafts and promote venous return. • Orthostatic intolerance or pain in lower extremities in a dependent position. • Initially assistive device to ambulate.
- 32. Scar management
- 34. Follow up care