
Recommended
More Related Content
What's hot
What's hot (18)
Similar to CLASSIFICATION OF ISCHEMIC HEART FAILURE SYNDROMES
Similar to CLASSIFICATION OF ISCHEMIC HEART FAILURE SYNDROMES (20)
More from asadsoomro1960
More from asadsoomro1960 (20)
Recently uploaded
Recently uploaded (20)
CLASSIFICATION OF ISCHEMIC HEART FAILURE SYNDROMES
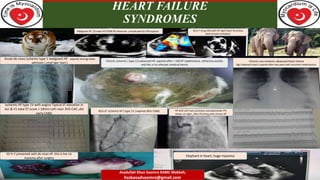
- 1. HEART FAILURE SYNDROMES World HEART FAILURE WORLD Chronic non ischemic advanced Heart Failure Big ( elephant heart ) expired after two years with recurrent readmissions. Acute de-novo ischemic type 1 malignant HF . expired during index admission ( small tiger heart ) Chronic ischemic ( type 11) advanced HF ,expired after > 100 HF readmissions ,refractory ascites and this is his infected umblical hernia RCA of Ischemic HF ( type 1V ) expired after CABG Malignant HF ,33 male Inf STEMI RV extension ,complicated by VSR expired . 30 yr F Cong VSD with HF right heart thrombus died of pulm embolism HF with Left main occlusion and polymorph VT( shown on right., after PCI living with chronic HF Ischemic HF type 1V with angina Typical ST elevation in Avr & V1 total ST score > 18mm Left main 3VD CAD ,did early CABG 50 Yr F presented with de novo HF .this is her LA myxoma after surgery Elephant in heart, huge myxoma Asadullah Khan Soomro KAMC Makkah; hssbasadsoomro@gmail.com
- 2. Introduction Heart Failure is not a disease itself but a complex and costly life threatening syndrome with multiple etiologies & precipitants. At present ,approximately 60 million worldwide are living with heart failure. 83 % of HF patients are hospitalized due to an acute HF episode at least once, and nearly half (43%) are hospitalized at least four times. Every year, there are approximately one million hospitalizations due to HF in the US and Europe, and on average, a HF patient remains in hospital for 5 to 10 days. Due to this, heart failure presents a major and growing health-economic burden that currently costs the world economy $108 billion every year
- 3. Cont, The out look for such patients is poor, with survival rates worse than many cancers. Furthermore ,heart failure has tremendous impact on patients, families, caregivers and healthcare system indeed, and is predicted to increase dramatically over the next decades to come. Heart failure is a major public health problem with high morbidity and mortality. Ischemic heart failure is commonest cause of heart failure all over the world and in kingdom of Saudi Arabia indeed ,however despite being common has never been classified appropriately.
- 5. SOOMRO,S , CLASSIFICATION OF ISCHEMIC HEART FAILURE SYNDROMES ISCHEMIC HEART FAILURE WITH MYOCARDIAL INFARCTION. 4 3 ISCHEMIC HEART FAILURE WITHOUT MYOCARDIAL INFARCTION. Subjective & objective evidence of healed ( Old ) myocardial infarction, complicated by first time or recurrent heart failure & hospitalization. 2 Subjective & objective evidence of acute myocardial infarction, complicated by heart failure during index hospitalization. 1 Primary symptoms of heart failure, without symptoms of angina and myocardial infarction ( Neither objective evidence of MI ). Concomitant symptoms of angina and heart failure, without subjective or objective evidence of myocardial infarction. ( Type 1 to type 1V )
- 6. Type 1V “ Orphan Ischemic heart failure Syndromes” “ Occlusion versus Stenosis” “ Myth or reality”
- 7. Ischemic Type 1V Heart failure syndromes ( Without MI & angina) Athero-thrombotic CAD is commonest cause of heart failure syndromes and is present in 2/3 of patients with heart failure and low ejection fraction. No controlled trials have addressed the issue of weather the coronary revascularization can improve clinical outcome in patients with heart failure without angina. However observational studies have shown that revascularization can favorably affect LV function in some patients with impaired yet viable myocardium.
- 8. Ischemic Type 1V Heart failure syndromes ( Without MI & angina) It is not clear how such patients should be identified because the sensitivity and specificity of abnormal imaging test have not been validated in patients with heart failure without angina. Additional studies are needed to determine weather the possibility of myocardial ischemia or viability should be evaluated routinely to assess the contribution of CAD in patients with HF and systolic dysfunction, who do not have angina 2004 HF Guide line recommends revascularization in patients with significant left main and in patients who have large area of non infarcted but hypoperfused and hypocontractile myocardium on non invasive testing.
- 9. Ischemic Type 1V Heart failure syndromes ( Without MI & angina) How should cardiac physician evaluate patients with heart failure, and LV systolic dysfunction ,who do not have chest pain and ,who do not have history of CAD indeed ??
- 10. Ischemic Type 1V Heart failure syndromes ( Without MI & angina) In younger patients without risk factors it is reasonable to exclude presence of congenital coronary anomalies. In older patients ,however efforts to detect the presence of CAD may not be worthwhile , because revascularization has not been shown to improve clinical outcomes in patients with heart failure without angina .
- 11. Ischemic Type 1V Heart failure syndromes ( Without MI & angina) Nevertheless , the observation that revascularization might have a favorable effect on LV function, has led some experts to suggest that CAD should be excluded whenever possible , especially in patients with DM , HTN, smokers and in those associated with silent myocardial ischemia. Only CAG can reliably demonstrate or exclude presence of significant CAD with good or bad targets of revascularization.
- 12. Why Ischemic Type 1V Heart failure syndromes are neglected. 1) Very Elderly patients with low ejection fraction are not studied to rule out CAD as cause of heart failure . 2) Similarly elderly hypertensive patients with perserved systolic function are usually neglected indeed .Therefore CAD as a cause of heart failure is overlooked. 3) Heart failure with global systolic dysfunction and LBBB despite having athero-thrombotic risk factors are also neglected as dilated / Ischemic cardiomyopathy and are presumed not suitable for coronary angiography, or delayed , and hence do not benefit from late revascularization.
- 13. Cont, 4) Elderly DM,HTN & CKD ,COPD with MR & TR associated with paroxysmal or permanent atrial fibrillation , and low ejection fraction are denied coronary angiography to rule out CAD as cause of heart failure until present with acute STEMI. 5) Adults with Corrected congenital heart defects , with residual sequele ,baseline abnormal EKG and ventricular dysfunction especially those associated metabolic syndrome , are also overlooked to rule out CAD as a etiology or precipitant of heart failure.
- 14. Cont, 6) Last not the least although rare but yet we see some patients with long standing risk factors , who are presented with malignant cardiac dysrrhythmias and first time symptoms of heart failure , with severe transient LV systolic dysfunction ,resuscitated successfully from cardiac arrest, with out EKG evidence of myocardial infarction . They are also neglected or delayed to rule out significant CAD with otherwise viable and good targets of revascularization.
- 15. Ischemic Type 1V Heart failure syndromes History , EKG and Echocardiogram ,found evidence of CAD in 42% men and 25% women predicting HF. However careful history in patients with high probability of CAD may help in diagnosis of type 1V ischemic heart failure in many patients. More recent studies using different techniques have found higher prevalence of type 1V ischemic heart failure syndromes . Average 61% ( 68% in men & 38% in women) in east Finland.
- 16. Ischemic Type 1V Heart failure syndromes In 1995 while working at Dow Medical college & civil hospital Karachi Pakistan, I first time discovered this tiny group of ischemic heart failure patients, who were presumed as dilated / ischemic cardiomyopathy but without objective evidence of CAD. They had severe LV systolic dysfunction with recurrent HF hospitalizations. ( dual reason ischemia as etiology of HF & precipitant of ADCHF without angina , EKG changes and troponin )
- 17. Ischemic Type 1V Heart failure syndromes To establish HF etiology ,and with a view to assess if they have suitable revascularization targets, we did coronary angiogram in few such high risk patients. We found in them small caliber ,multi vessel severe diffuse ,multiple lesions ,( as an ischemic etiology and precipitant of decompensation indeed). Considered unsuitable for revascularization , therefore stopped further testing .
- 18. Ischemic Type 1V Heart failure syndromes Based on above coronary morphological features and diverse clinical manifestations , I first time in 1995 classified ischemic heart failure in four groups. I presented a first paper on heart failure audit in Dow medical golden jubilee and centenary scientific congress held on 28th December 1996 and in cardiology congress organized by Pakistan cardiac society , but was categorically neglected by most of the physicians.
- 19. Ischemic Type 1V Heart failure syndromes After coming to Kingdom of Saudi Arabia in 2002 , continued interest in ischemic heart failure syndromes, after joining prince sultan cardiac center in Al - Ahsa in 2007 ,after around 15 year ,again I discovered few patients with ischemic type 1V heart failure syndromes with same coronary morphological features. Following is one of the good example to share in this regard.
- 20. THANK YOU Living Longer, Living Well