
Recommended
More Related Content
What's hot
Similar to Chronic pulmonary disorder - ASTHMA
Similar to Chronic pulmonary disorder - ASTHMA (20)
Recently uploaded
Recently uploaded (20)
Chronic pulmonary disorder - ASTHMA
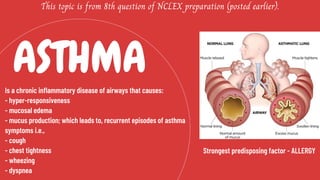
- 1. ASTHMA This topic is from 8th question of NCLEX preparation (posted earlier). Is a chronic inflammatory disease of airways that causes: - hyper-responsiveness - mucosal edema - mucus production; which leads to, recurrent episodes of asthma symptoms i.e., - cough - chest tightness - wheezing - dyspnea Strongest predisposing factor - ALLERGY
- 2. • It involves inflammatory and structural cells:- (a) Mast cells - when activated, release chemicals i.e. called MEDIATORS. (b) Macrophages (c) T - lymphocytes (d) Neutrophils (e) Eosinophils Perpetuate inflammatory response. 1) Histamine 2) Leukotrienes 3) Bradykinine 4) Prostanoids 5) Cytokines • Increased blood flow • Vasoconstriction • Fluid leak from vasculature • Accumulation of WBC's to the area • Mucus secretion • Brocncho constriction • Bronchoconstriction results from IgE-dependent release of mediators from mast cells. This directly contract the airway.
- 3. Cough [with/without mucus] Dyspnea Wheezing EARLY LATE Diaphoresis Tachycardia Widened pulse pressure Hypoxemia Central cyanosis [late sign of poor oxygenation]
- 4. 1) Mild intermittent. • Symptoms 2/fewer times each week. • Brief exacerbation. • Nighttime symptoms 2/fewer times each month. • Symptoms more than 2 times/week, but less than once a day. • Exacerbation affect activity. • Night time symptoms more than twice/month. • Daily symptoms. • Frequent night time symptoms. • Limited physical activity. • Continual symptoms. • Frequent exacerbation. • Limited physical activity. • Frequent night time symptoms. 2) Mild persistent. 3) Moderate persistent. 4) Severe persistent.
- 5. - Determine presence of: • episodic symptoms of airflow obstruction. • airflow atleast partially reversible. - Positive family history. - Environmental factors: • seasonal changes • high pollen counts • climate changes • air pollution - Occupation related chemicals, foods and compounds. - Co-morbid conditions that may accompany asthma: • GERD • drug-induced asthma • allergic broncho pulmonary aspergillosis - Other allergic reactions can be: • eczema • rashes • temporary edema - DURING ACUTE EPISODES: 1) Sputum & blood tests- increased level of eosinophils. 2) Increased serum level of IgE. 3) ABG analysis & pulse oximetry - hypoxemia. 4) Increased PaCO2 - worsening condition (pt. becomes fatigues). 5) Spirometry - evaluate lung capacity.
- 6. 1) Status asthmaticus 2) Respiratory failure 3) Pneumonia 4) Atelectasis 5) Hypoxemia
- 7. 2 general classes of asthma Long acting medication Quick relief medication 1) Short acting beta2 adrenergic agonists: - Albuterol - Levalbuterol - Pirbuterol 2) Anticholinergics: - Inhibits muscarinic cholinergic receptors. - Reduce intrinsic vagal tone of the airway. - Ipratopium 1) Corticosteroids: - most potent. - anti-inflammatory medication. - Functions:- a) reduce symptoms. b) improve airway functions. c) reduce peak flow variability. 2) Cromolyn sodium and nedocromil: - mild to moderate anti- inflammatory. - alternative med. to treament. - Functions:- a) stabilize mast cells. b) effective on prophylactic basis. - CONTRAINDICATED in Acute Asthma Exacerbations.
- 8. 3) Long acting beta2 adrenergic agonists: - used with anti-inflammatory med. to control asthma symptoms. - Functions:- a) prevent exercise induced asthma [not recommended for immediate relief of symptoms.] 4) Theophylline: - mild to moderate bronchodilator. used in addition to inhaled corticosteroids. 5) Salmeterol & formoterol: - used in other med. in long term control of asthma. - bronchodilate for atleast 24 hours. 6) Anti-leukotrienes: - Inhibitors - Montelukast - Zafirlukast - Zileuton 7) Immuno modulators: - Functions:- a) prevent binding of IgE to the high affinity receptors of basophils and mast cells. b) Omalizumab- monoclonal antibody.
- 9. - Peak flow meters measure the highest airflow during a forced expiration. - The patient is indtructed in proper techniques. - Peak flow are monitored for 2-3 weeks after receipt of optimal asthma therapy. The patient's 'personal best' value is measured. - Zones that are determined: 1) Green : 80% - 100% 2) Yellow: 60% - 80% 3) Red: less than 60%
- 10. Thank you!