1. EVALUATION OF IMPLANTING SPINAL CORD STIMULATORS IN PATIENTS
WITH OTHER IMPLANTED DEVICES
Lee S, Sachdeva H, Abd-Elsayed A
Department of Anesthesiology, University of Cincinnati, Cincinnati, Ohio
Introduction:
Spinal cord stimulators (SCS) have been used since 1967 to
successfully treat many chronic pain conditions (1). Implantable
electrical devices such as cardioverter-defibrillators, gastric
pacemakers, intrathecal drug delivery pumps, and deep brain
stimulators are becoming increasingly common with the expanding
efficacy of these devices. There has been concern that having multiple
devices that use electrical impulses implanted in the same patient may
lead to failure of one or both systems or inappropriate impulses from
the second device in response to stimulation from the SCS if there is
electromagnetic interference or cross-talk between the two devices
(2). We present three patients with a SCS and another implantable
electrical device.
Case Presentation:
Case 1: A 77 year old man presented with chronic lumbar back pain
since the late 1980’s. He had undergone numerous treatment
modalities including pain medications, physical therapy, chiropractic
treatment, massage therapy, multiple epidural injections, and back
surgery without significant improvement in pain. The patient also had
congestive heart failure requiring implantation of a St. Jude single
chamber defibrillator 9 years ago. The patient was not a candidate for
repeat back surgery and given his failed conservative therapy, a trial of
SCS was recommended. The patient experienced greater than 50%
improvement in pain and a permanent St. Jude SCS was implanted.
The patient’s automatic ICD was monitored by the anesthesia team
during the entire case. At 3 weeks follow up, patient stated pain was
improved by more than 70%. He was able to walk, stand longer, and
perform his daily activities once again. The patient has had both a
SCS and ICD for 5 months without reported failure of either system.
Case 2: The patient is an 89 year old man who presented for chronic
back pain of nearly 60 years that has been refractory to numerous
treatment modalities including physical therapy, epidural steroid
injections, medial branch block, facet join injection, and radiofrequency
ablation. Of note, a Medtronic pacemaker was implanted 8 months
ago due to bradycardia and syncope. Patient was not a candidate for
back surgery due to his co-morbidities so a trial of a Medtronic SCS
was recommended. The patient’s pain did not improve with the trial of
SCS, as the stimulation was too strong in his legs. Despite
reprogramming, it was still unable to provide coverage of his lower
back without affecting his legs and the trial was discontinued. He will
reconsider another SCS trial in the future if necessary. The patient’s
pace maker was unaffected by the SCS and continued to function as
intended during the trial period.
Case 3: A 59 year old woman presented for evaluation of possible
addition of leads to her SCS to provide increased coverage of right
knee pain in addition to her lower back. The patient’s back pain
began 15 years ago was unresolved with conservative treatment. After
undergoing 2 failed back surgeries 11 and 12 years ago, she was
recommended SCS and after a successful trial had a permanent SCS
implanted with significant pain relief that allowed her to resume her
daily activities. However, the patient required total right knee
replacement 4 years ago and has had pain in that knee since then.
Two Boston Scientific octad leads were added to her SCS coverage
successfully including her right knee. Pain relief in her back and right
knee was 90% and she was able to again perform her daily activities.
She then had implantation of a bladder stimulator for urinary
incontinence 2 years ago. The patient has not had any issues with her
bladder stimulator since she has had both the bladder stimulator and
SCS.
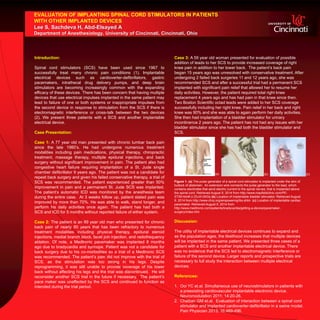
Figure 1. (a) The pulse generator of a spinal cord stimulator is implanted under the skin of
buttock of abdomen. An extension wire connects the pulse generator to the lead, which
contains electrodes that send electric current to the spinal nerves, that is implanted above
the spinal cord. Retrieved August 9, 2014 from http://www.mayfieldclinic.com/PE-
STIM.htm#.U-ZhJ41dXGs (b) Location of implantable bladder stimulator. Retrieved August
9, 2014 from http://www.chrp.org/empowering/ibs.shtm (c) Location of implantable cardiac
pacemaker. Retrieved August 9, 2014 from
http://www.medtronic.com/patients/bradycardia/getting-a-device/pacemaker-
surgery/index.htm
Discussion:
The utility of implantable electrical devices continues to expand and
as the population ages, the likelihood increases that multiple devices
will be implanted in the same patient. We presented three cases of a
patient with a SCS and another implantable electrical device. There
was no evidence that the SCS led to electromagnetic interference or
failure of the second device. Larger reports and prospective trials are
necessary to full study the interaction between multiple electrical
devices.
References:
1. Ooi YC et.al. Simultaneous use of neurostimulators in patients with
a preexisting cardiovascular implantable electronic device.
Neuromodulation 2011; 14:20-26.
2. Chaiban GM et.al. Evaluation of interaction between a spinal cord
stimulator and implanted cardioverter-defibrillator in a swine model.
Pain Physician 2013; 16:489-496.
(b) (c)(a)