Type 2 Diabetes Patient Care Decision Cycle Guide
•
0 likes•144 views

John E. Anderson, MD, prepared useful practice aids pertaining to type 2 diabetes for this CME activity titled "Realizing Your Patient’s Potential: Embracing the Guidelines to Appropriately Individualize Care for Patients With Type 2 Diabetes." For the full presentation, monograph, complete CME information, and to apply for credit, please visit us at http://bit.ly/2UlgLL0. CME credit will be available until April 16, 2020.

Recommended
Recommended
More Related Content
What's hot
What's hot (19)
Similar to Type 2 Diabetes Patient Care Decision Cycle Guide
Similar to Type 2 Diabetes Patient Care Decision Cycle Guide (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Type 2 Diabetes Patient Care Decision Cycle Guide
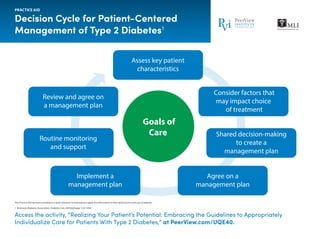
- 1. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. Decision Cycle for Patient-Centered Management of Type 2 Diabetes1 1. American Diabetes Association. Diabetes Care. 2019;42(Suppl 1):S1-S193. PRACTICE AID Access the activity, “Realizing Your Patient’s Potential: Embracing the Guidelines to Appropriately Individualize Care for Patients With Type 2 Diabetes,” at PeerView.com/UQE40. Assess key patient characteristics Consider factors that may impact choice of treatment Shared decision-making to create a management plan Agree on a management plan Implement a management plan Routine monitoring and support Review and agree on a management plan Goals of Care
- 2. Access the activity, “Realizing Your Patient’s Potential: Embracing the Guidelines to Appropriately Individualize Care for Patients With Type 2 Diabetes,” at PeerView.com/UQE40. Assessing Patient Characteristics: Key Components of the Comprehensive Diabetes Medical Evaluation1 This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. PRACTICE AID Psychosocial conditions • Screen for depression, anxiety, and disordered eating; refer for further assessment or intervention if warranted • Identify existing social supports • Consider assessment for cognitive impairmenta Diabetes self-management education and support • History of dietitian/diabetes educator visits/classes • Assess diabetes self-management skills and barriers • Assess familiarity with carbohydrate counting (type 1 diabetes) Pregnancy planning • For women with childbearing capacity, review contraceptive needs and preconception planning Behavioral and Diabetes Self- Management Skills Initial Visit Every Follow-Up Visit Annual Visit Diabetes history Components of the Comprehensive Diabetes Medical Evaluation at Initial, Follow-Up, and Annual Visits • Characteristics at onset (eg, age, symptoms) • Review of previous treatment regimens and response • Assess frequency/cause/severity of past hospitalizations Family history • Family history of diabetes in a first-degree relative • Family history of autoimmune disorder Personal history of complications and common comorbidities • Macrovascular and microvascular • Common comorbidities (eg, obesity, OSA) • Hypoglycemia: awareness/frequency/causes/timing of episodes • Presence of hemoglobinopathies or anemias • High blood pressure or abnormal lipids • Last dental visit • Last dilated eye exam • Visits to the specialist Interval history • Changes in medical/family history since last visit • Eating patterns and weight history • Physical activity and sleep behaviors • Tobacco, alcohol, and substance use • Current medication regimen • Medication-taking behavior • Medication intolerance or side effects • Complementary and alternative medicine use • Vaccination history and needs • Assess use of health apps, online education, patient portals, etc • Glucose monitoring (meter/CGM): results and data use • Review insulin pump settings and use This Visit Lifestyle Factors Past Medical and Family History Medications and Vaccinations Technology Use
- 3. Access the activity, “Realizing Your Patient’s Potential: Embracing the Guidelines to Appropriately Individualize Care for Patients With Type 2 Diabetes,” at PeerView.com/UQE40. Assessing Patient Characteristics: Key Components of the Comprehensive Diabetes Medical Evaluation1 This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. ABI: ankle-brachial pressure index; ACE: angiotensin-converting enzyme; ARB: angiotensin receptor blocker; CGM: continuous glucose monitors; OSA: obstructive sleep apnea; PAD: peripheral arterial disease. a At 65 years of age or older. b Should be performed at every visit in patients with sensory loss, previous foot ulcers, or amputations. c May also need to be checked after initiation or dose changes of medications that affect these laboratory values (ie, diabetes medications, blood pressure medications, cholesterol medications, or thyroid medications). d In people without dyslipidemia and not on cholesterol-lowering therapy, testing may be less frequent. e May be needed more frequently in patients with known chronic kidney disease or with changes in medications that affect kidney function and serum potassium. 1. American Diabetes Association. Diabetes Care. 2019;42(Suppl 1):S1-S193. PRACTICE AID Initial Visit Every Follow-Up Visit Annual Visit • Height, weight, and BMI; growth/pubertal development in children and adolescents • Blood pressure determination • Orthostatic blood pressure measures (when indicated) • Fundoscopic examination (refer to eye specialist) • Thyroid palpation • Skin examination (eg, acanthosis nigricans, insulin injection or insertion sites, lipodystrophy) • Comprehensive foot examination – Visual inspection (eg, skin integrity, callous formation, foot deformity or ulcer, toenails)b – Screen for PAD (pedal pulses; refer for ABI if diminished) – Determination of temperature, vibration or pinprick sensation, and 10-g monofilament exam • A1C, if the results are not available within the past 3 months • If not performed/available within the past year – Lipid profile, including total, LDL, and HDL cholesterol and triglyceridesc – Liver function testsc – Spot urinary albumin-to-creatinine ratio – Serum creatinine and estimated glomerular filtration ratee – Thyroid-stimulating hormone in patients with type 1 diabetesc – Vitamin B12 if on metformin (when indicated) – Serum potassium levels in patients on ACE inhibitors, ARBs, or diureticse d Physical Examination Laboratory Evaluation American Diabetes Association Standards of Medical Care App • Download on the App Store for IOS • Download on Google Play for Android This Visit
- 4. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. 1. Unger J. Diabetes Metab Syndr Obes. 2012;5:57-74. PRACTICE AID Access the activity, “Realizing Your Patient’s Potential: Embracing the Guidelines to Appropriately Individualize Care for Patients With Type 2 Diabetes,” at PeerView.com/UQE40. • When did the event(s) occur? (daytime versus overnight) • Under what circumstances did they occur? (missed meal, following exercise, excess medication) • What were the symptoms? • What was done? (eg, carbohydrates ingested, follow-up blood glucose monitoring) • What was the blood glucose reading? • Did they require assistance from another person in order to reverse the hypoglycemia? • With whom and how did they treat the hypoglycemia? • How soon did hypoglycemia resolve? (blood glucose levels rose to 3.9 mmol/L [70 mg/dL]) • Did the hypoglycemic event reoccur later within a 24-hour period? • How fearful is the patient or the family of hypoglycemia? • Do they test their glucose level before driving? • Does the patient “stack insulin” (re-bolus rapid insulin analog within 3 hours of a similar injection)? • At what glycemic level does the patient perceive hypoglycemia? (If 50 mg/dL, patient may have hypoglycemia-associated autonomic failure.) • Does the patient understand the consequences of hypoglycemia? (Some patients prefer being “low” rather than “high” because they fear the consequences of acute or chronic hyperglycemia.) Talking With Patients About Hypoglycemic Events1
- 5. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. Diabetes Management Resources VA: Veterans Affairs. PRACTICE AID Access the activity, “Realizing Your Patient’s Potential: Embracing the Guidelines to Appropriately Individualize Care for Patients With Type 2 Diabetes,” at PeerView.com/UQE40. Resource URL American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Type 2 Diabetes Management Algorithm 2019 https://journals.aace.com/doi/pdf/10.4158/CS-2018-0535 American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) Consensus Statement—2018 http://care.diabetesjournals.org/content/diacare/41/12/2669.full.pdf ADA Standards of Medical Care—2019 https://professional.diabetes.org/content-page/practice-guidelines-resources ADA Standards of Medical Care in Diabetes—2019 Abridged for Primary Care Providers http://clinical.diabetesjournals.org/content/diaclin/early/2018/12/16/cd18-0105.full.pdf ADA Standards of Medical Care App https://professional.diabetes.org/content-page/standards-care-app-1 US Dietary Guidelines (MyPlate) https://health.gov/dietaryguidelines/2015/resources/2015-2020_Dietary_Guidelines.pdf VA MOVE!® Coach app https://mobile.va.gov/app/move-coach Osteoarthritis Education https://arthritisaustralia.com.au/ Mayo Clinic Diabetes Decision Aids Downloadable brochures and instructions: https://shareddecisions.mayoclinic.org/decision-aid- information/decision-aids-for-chronic-disease/diabetes-medication-management/ Video demonstration: https://www.youtube.com/watch?v=SYTPqceFgSw Medication availability https://info.mmitnetwork.com/formulary-search https://lookup.decisionresourcesgroup.com/ https://mobile.va.gov/app/ask-a-pharmacist https://www.goodrx.com/