Overcoming Challenges in the Recognition and Management of Adult ADHD in Primary Care: Optimizing Outcomes to Reduce Disease Burden and Improve Quality of Life
•
0 likes•55 views

Co-Chairs, Lenard A. Adler, MD, and Oren Mason, MD, prepared useful Practice Aids pertaining to ADHD for this CME activity titled “Overcoming Challenges in the Recognition and Management of Adult ADHD in Primary Care: Optimizing Outcomes to Reduce Disease Burden and Improve Quality of Life.” For the full presentation, downloadable Practice Aids, and complete CME information, and to apply for credit, please visit us at https://bit.ly/3kMSUjb. CME credit will be available until December 22, 2022.

Recommended
Recommended
More Related Content
Similar to Overcoming Challenges in the Recognition and Management of Adult ADHD in Primary Care: Optimizing Outcomes to Reduce Disease Burden and Improve Quality of Life
Similar to Overcoming Challenges in the Recognition and Management of Adult ADHD in Primary Care: Optimizing Outcomes to Reduce Disease Burden and Improve Quality of Life (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Overcoming Challenges in the Recognition and Management of Adult ADHD in Primary Care: Optimizing Outcomes to Reduce Disease Burden and Improve Quality of Life
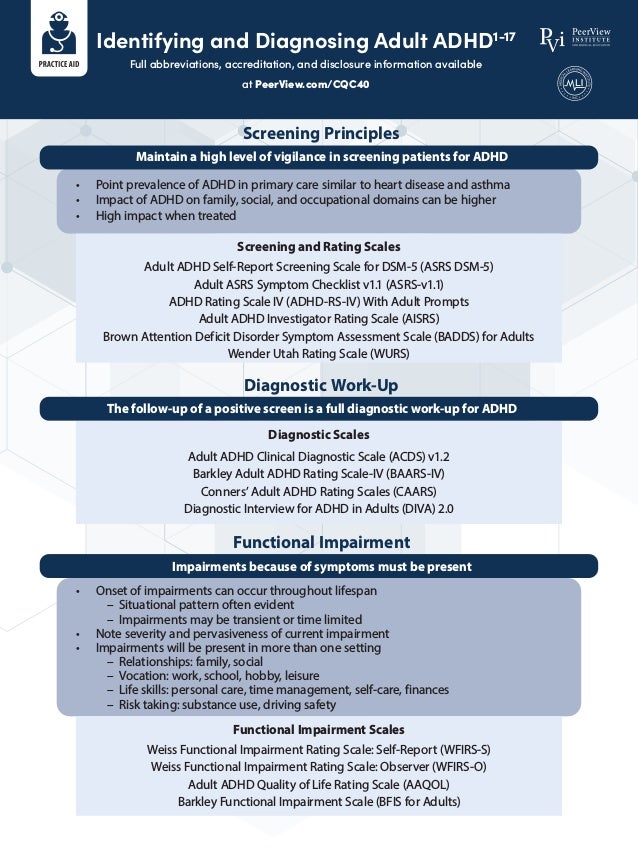
- 1. Identifying and Diagnosing Adult ADHD1-17 Full abbreviations, accreditation, and disclosure information available at PeerView.com/CQC40 Screening Principles Functional Impairment Diagnostic Work-Up Maintain a high level of vigilance in screening patients for ADHD Impairments because of symptoms must be present The follow-up of a positive screen is a full diagnostic work-up for ADHD Screening and Rating Scales Functional Impairment Scales Diagnostic Scales • Point prevalence of ADHD in primary care similar to heart disease and asthma • Impact of ADHD on family, social, and occupational domains can be higher • High impact when treated • Onset of impairments can occur throughout lifespan – Situational pattern often evident – Impairments may be transient or time limited • Note severity and pervasiveness of current impairment • Impairments will be present in more than one setting – Relationships: family, social – Vocation: work, school, hobby, leisure – Life skills: personal care, time management, self-care, finances – Risk taking: substance use, driving safety Adult ADHD Self-Report Screening Scale for DSM-5 (ASRS DSM-5) Adult ASRS Symptom Checklist v1.1 (ASRS-v1.1) ADHD Rating Scale IV (ADHD-RS-IV) With Adult Prompts Adult ADHD Investigator Rating Scale (AISRS) Brown Attention Deficit Disorder Symptom Assessment Scale (BADDS) for Adults Wender Utah Rating Scale (WURS) Weiss Functional Impairment Rating Scale: Self-Report (WFIRS-S) Weiss Functional Impairment Rating Scale: Observer (WFIRS-O) Adult ADHD Quality of Life Rating Scale (AAQOL) Barkley Functional Impairment Scale (BFIS for Adults) Adult ADHD Clinical Diagnostic Scale (ACDS) v1.2 Barkley Adult ADHD Rating Scale-IV (BAARS-IV) Conners’ Adult ADHD Rating Scales (CAARS) Diagnostic Interview for ADHD in Adults (DIVA) 2.0
- 2. Identifying and Diagnosing Adult ADHD1-17 Full abbreviations, accreditation, and disclosure information available at PeerView.com/CQC40 ADHD Diagnostic Process Schedule adequate time Preparation prior to visit • Two 30-minute visits (CPT 99214; eg, consecutive days) • Alternately: 60-minute visit (CPT 99215 or 90801) • Structured questionnaires completed prior to appointment; at minimum, consider – Adult ADHD Self-Report Scale: 18 items – Weiss Functional Impairment Rating Scale: Self-Report • Screeners: anxiety, depression, mood disorder, SUD • Establish time course of ADHD symptoms – Long-standing, not episodic • Catalogue impairments because of symptoms – Often situational or time limited – Relevant past history (eg, prior SUD, legal issues) • Diagnostic screeners for comorbid disorders – Interview – Hamilton Depression Rating Scale (HDRS) – Hamilton Anxiety Rating Scale (HAM-A) – CAGE Questionnaire (CAGE-AID) – Mood Disorder Questionnaire (MDQ) • Establish diagnosis with patient • Cardiovascular baseline screening • Disease-state education • Define patient’s therapy goals – “What three changes would you most like to see as a result of therapy?” • Initiate therapy – Medication trial of therapy – Psychosocial support – Accommodations • Schedule follow-up in 1 month • Remember to – Identify medical comorbidities and medications that may impair cognitive function or exclude patient from ADHD treatment – Request collateral information about medical history from someone close to patient Visit 1 Visit 2
- 3. Identifying and Diagnosing Adult ADHD1-17 Full abbreviations, accreditation, and disclosure information available at PeerView.com/CQC40 Comorbid Psychiatric Disorders Are Very Common The following psychiatric disorders have elevated rates in adults with ADHD Psychiatric screeners for adults The following should NOT be used to dismiss a diagnosisof ADHD • Bipolar disorder • Major depressive disorder • Substance use disorder • Hamilton Depression Rating Scale (HDRS) • Hamilton Anxiety Rating Scale (HAM-A) • CAGE Questionnaire (CAGE-AID) • Mood Disorder Questionnaire (MDQ) • The clinician does not observe hyperactivity in the office • There is no family history of ADHD • The patient – Has past or current anxietyor depression – Is sedentary with sluggish mannerisms – Is quiet or shy or has a reticent personality – Is well educated or employed in a high-level position – Is financially success ful – Is well mannered, has a stylish appearance, or has polished social skills – Showed clear signs of hyperactivity, impulsivity, andinattention in childhood but has difficulty only with residualsymptoms now – Does not remember or denies symptoms in childhood,and school records are unavailable • Anxiety disorders • Personality disorders 1. Kessler RC et al. Arch Gen Psychiatry. 2010;67:1168-1178. 2. Goodman DW. Prim Psychiatry. 2009;16:21-30. 3. Barkley RA. Barkley Adult ADHD Rating Scale—IV (BAARS-IV). New York, NY: Guilford Press; 2011. 4. Conners KC et al. (CAARS) Conners' Adult ADHD Rating Scales. Torrance, CA: WPS Publishing; 1998. 5. https://www.advancedassessments.co.uk/resources/ADHD-Screening-Test-Adult.pdf. 6. https://nyulangone.org/files/psych_adhd_checklist_0.pdf. 7. https://www.hcp.med.harvard.edu/ncs/ftpdir/adhd/ASRS-5_English.pdf. 8. Adler LA et al. In: Adler LA et al, eds. Attention-Deficit Hyperactivity Disorder in Adults and Children. Cambridge, UK: Cambridge University Press; 2015:224-232. 9. DuPaul GJ et al. ADHD Rating Scale-IV: Checklists, Norms, and Clinical Interpretation. New York, NY: Guilford Press; 1998. 10. Spencer TJ et al. J Atten Disord. 2010;14:57-68. 11. Brown T. Brown Attention-Deficit Disorder Scales. Boston, MA: Springer; 2011. 12. http://neurosciencecme.com/library/rating_scales/ adhd_wender.pdf. 13. http://www.shared-care.ca/files/Weiss_Functional_Impairment_Self-Report.pdf. 14. Canu WH et al. J Atten Disord. 2020;24:1648-1660. 15. Brod M et al. Atten Defic Hyperact Disord. 2015;7:141-150. 16. Barkley RA. Barkley Functional Impairment Scale (BFIS for Adults). New York, NY: Guilford Press; 2011. 17. Katzman MA et al. BMC Psychiatry. 2017;17:302.
- 4. Shared Decision-Making in ADHD1-9 Full abbreviations, accreditation, and disclosure information available at PeerView.com/CQC40 The Role of the Clinician and Patient in Shared Decision-Making Clinician Patient Provides evidence-based information/education Informs about risks involved with each option Has professional expertise Trusts patient’s worldview and values patient experiences, thereby building therapeutic alliance Presents multiple treatment options with risks and benefits of each, so that patient is active participant rather than passive in selecting treatment Has lived-experience expertise Clarifies and aligns decisions with goals Shares values and preferences to promote mutual understanding Barriers for Clinicians and Patients in Shared Decision-Making Takes personal accountability for medical decisions, including those about medications and types of therapies Includes families/caregivers to facilitate SDM and help to enact the treatment plan Lack of time Stigma about mental illness inhibiting open communication and willingness to consider medication Believing patients have low capacity to make decisions Provider’s own treatment preference Patients not advocating for their own involvement Less experience (less provider experience is associated with lower patient involvement) Not having been provided the option to participate in shared decision-making Lack of structural support Not wanting to make the final decision Clinician Patient
- 5. Shared Decision-Making in ADHD1-9 Full abbreviations, accreditation, and disclosure information available at PeerView.com/CQC40 The Key Components of Engaging Patients in the Decision-Making Process 1. Introduce choice 2. Describe options 3. Help make decisions Identify/summarize problem Offer choices Emphasize importance of personal preferences Discuss any uncertainties in treatment Check reaction Defer final decision until you are able to discuss options in more detail if patient asks, “What would you do?” Determine what the patient already knows List and describe options including risks and benefits of stimulant and nonstimulant medications for the treatment of ADHD Provide decision support such as decision aids, which can help patients understand their options List options again and apply teach-back method by asking patient how they would describe the options to a loved one Focus on preferences Check to see if patient is ready to make a decision or if they need more time or have additional questions Agree on treatment plan Ensure patient understands that the plan can be modified and decisions can be reviewed at any time 1. Slade M. World Psychiatry. 2017;16:146-153. 2. Zisman-Ilani Y et al. JAMA Psychiatry. 2021;78:1183-1184. 3. Da Costa H et al. J Nerv Ment Dis. 2020;208:329-339. 4. Guidry-Grimes L. AMA J Ethics. 2020;22:E446-E451. 5. Maples NJ et al. Community Ment Health J. 2021 June 27 [Epub ahead of print]. 6. Farrelly S et al. Health Expect. 2015;19:448-458. 7. Rodenburg-Vandenbussche S et al. J Eval Clin Pract. 2020;26:645-658. 8. Matthews EB et al. Front Psychiatry. 2021;12:681165. 9. Gravel K et al. Implement Sci. 2006;1:16.