Advances in the Treatment of Uncontrolled Persistent Asthma: Expert Insights in Personalizing Patient Care
•
0 likes•111 views

Michael E. Wechsler, MD, and Flavia C.L. Hoyte, MD, prepared useful practice aids pertaining to uncontrolled persistent asthma for this CME activity titled "Advances in the Treatment of Uncontrolled Persistent Asthma: Expert Insights in Personalizing Patient Care.” For the full presentation, monograph, complete CME information, and to apply for credit, please visit us at http://bit.ly/2YSAn7u. CME credit will be available until July 24, 2020.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Advances in the Treatment of Uncontrolled Persistent Asthma: Expert Insights in Personalizing Patient Care
Similar to Advances in the Treatment of Uncontrolled Persistent Asthma: Expert Insights in Personalizing Patient Care (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Advances in the Treatment of Uncontrolled Persistent Asthma: Expert Insights in Personalizing Patient Care
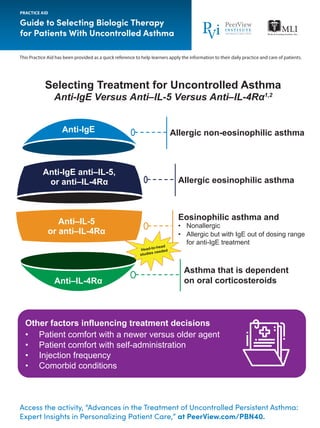
- 1. Access the activity, “Advances in the Treatment of Uncontrolled Persistent Asthma: Expert Insights in Personalizing Patient Care,” at PeerView.com/PBN40. Guide to Selecting Biologic Therapy for Patients With Uncontrolled Asthma PRACTICE AID This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. Other factors influencing treatment decisions • Patient comfort with a newer versus older agent • Patient comfort with self-administration • Injection frequency • Comorbid conditions Head-to-head studies needed Selecting Treatment for Uncontrolled Asthma Anti-IgE Versus Anti‒IL-5 Versus Anti‒IL-4Rα1,2 Anti-IgE anti–IL-5, or anti–IL-4Rα Anti–IL-5 or anti–IL-4Rα Anti–IL-4Rα Allergic non-eosinophilic asthma Allergic eosinophilic asthma Eosinophilic asthma and • Nonallergic • Allergic but with IgE out of dosing range for anti-IgE treatment Asthma that is dependent on oral corticosteroids Anti-IgE
- 2. Access the activity, “Advances in the Treatment of Uncontrolled Persistent Asthma: Expert Insights in Personalizing Patient Care,” at PeerView.com/PBN40. Guide to Selecting Biologic Therapy for Patients With Uncontrolled Asthma PRACTICE AID CRTh2: chemoattractant receptor-homologous molecule expressed on T-helper 2 cells; IgE: immunoglobulin E; IL: interleukin; IL-#R: interleukin-# receptor; TSLP: thymic stromal lymphopoietin. 1. Papathanassiou E et al. Eur Clin Resp J. 2016;3:31813. 2. Magnan A et al. Allergy. 2016;71:1335-1344. 3. Xolair (omalizumab) Prescribing Information. https://www.gene.com/download/pdf/xolair_ prescribing.pdf. Accessed June 10, 2019. 4. Nucala (mepolizumab) Prescribing Information. http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/125526Orig1s000Lbl.pdf. Accessed June 10, 2019. 5. Cinqair (reslizumab) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/761033lbl.pdf. Accessed June 10, 2019. 6. Fasenra (benralizumab) Prescribing Information. https://www.azpicentral.com/fasenra/fasenra_pi.pdf#page=1. Accessed June 10, 2019. 7. Dupixent (dupilumab) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_ docs/label/2017/761055lbl.pdf. Accessed June 10, 2019. 8. https://www.prnewswire.com/news-releases/ tezepelumab-granted-breakthrough-therapy-designation-by-us-fda-for-the-treatment-of-patients-with-severe-asthma-without-an-eosinophilic-phenotype-300708680.html. Accessed June 10, 2019. 9. https://clinicaltrials.gov/ct2/show/NCT03347279. Accessed June 10, 2019. 10. https://clinicaltrials.gov/ct2/show/NCT03406078. Accessed June 10, 2019. 11. Corren J et al. N Engl J Med. 2017;377:936- 946. 12. https://clinicaltrials.gov/ct2/show/NCT02563067. Accessed June 10, 2019. 13. https://clinicaltrials.gov/ct2/show/NCT03052517. Accessed June 10, 2019. 14. https://clinicaltrials.gov/ct2/show/ NCT02555683. Accessed June 10, 2019. Agent/Target Indication/Current Status Route/Dosing Patients aged ≥6 y with moderate to severe persistent allergic asthma inadequately controlled with inhaled corticosteroids Subcutaneous 75-375 mg every 2-4 weeks (dosage based on IgE level and body weight) Add-on maintenance treatment of patients aged ≥12 y with severe asthma and an eosinophilic phenotype Subcutaneous 100 mg every 4 weeks Add-on maintenance treatment of patients aged ≥18 y with severe asthma and an eosinophilic phenotype Intravenous infusion 3 mg/kg every 4 weeks over 20-50 minutes Add-on maintenance treatment of patients aged ≥12 y with severe asthma and an eosinophilic phenotype Subcutaneous 30 mg every 4 weeks for first 3 doses, then every 8 weeks Add-on maintenance treatment of patients aged ≥12 years with moderate to severe asthma with an eosinophilic phenotype or with oral corticosteroid-dependent asthma Subcutaneous Initial dose of 400 mg followed by 200 mg every 2 weeks or initial dose of 600 mg followed by 300 mg every 2 weeks Phase 3 trials; breakthrough designation for noneosinophilic phenotype Subcutaneous 210 mg every 4 weeks Phase 3 trials Oral Dupilumab7 IL-4Rα (IL-4/IL-13) Tezepelumab8-10 TSLP Fevipiprant11-14 CRTh2 Investigational Omalizumab3 IgE Mepolizumab4 IL-5 Reslizumab5 IL-5 Benralizumab6 IL-5Rα/βc Approved
- 3. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. What Is Eosinophilic Asthma?1 1. https://www.everydayhealth.com/hs/asthma/eosinophilic-asthma-essential-facts/. Accessed June 10, 2019. 2. Eng SS et al. Clin Rev Allergy Immunol. 2016;50:140-158. PRACTICE AID Access the activity, “Advances in the Treatment of Uncontrolled Persistent Asthma: Expert Insights in Personalizing Patient Care,” at PeerView.com/PBN40. Eosinophils play an important role in your immune system • Eosinophils are part of your immune system and may play a critical role in your body’s defense against bacterial, viral, fungal, and parasitic infections2 • They help promote inflammation, your body’s protective response to injury and infection, but too many can cause excess inflammation and swelling • Elevated levels of eosinophils have been associated with asthma and other conditions, such as atopic dermatitis Eosinophilic asthma often develops in adults • Individuals who develop severe asthma in adulthood are more likely to have the eosinophilic type • The condition is most commonly diagnosed in adults aged 35 to 50 years Up to half of severe asthma cases may be associated with eosinophils • About 50% of people with severe asthma may have elevated levels of eosinophils in their blood and lungs • Your asthma may be considered severe if – Your symptoms interfere with daily activities – You use your rescue inhaler frequently – Your symptoms don’t respond to typical asthma treatments taken regularly and correctly A blood test can help diagnose eosinophilic asthma • If you are having trouble controlling asthma symptoms despite following your treatment plan, talk to your doctor about getting tested for eosinophilic asthma • A simple blood test called eosinophil count can help diagnose eosinophilic asthma; your doctor may also recommend a sputum eosinophil count or a bronchial biopsy to help confirm diagnosis Eosinophilic asthma is associated with nasal polyps • People with eosinophilic asthma may have an increased risk of nasal polyps, or noncancerous growths, inside the nose New medications are available to treat eosinophilic asthma • Standard treatments for asthma include long-term controller medications and rescue medications that you use when your symptoms flare up • If these medications are not enough to control your asthma, your doctor may prescribe newer medications called biologics that target specific molecules involved in the action of eosinophils to help lower eosinophil levels and reduce inflammation; talk to your doctor about the treatment that’s right for you