Nursing Education: Appetite Stimulants for Elderly Patients
•
0 likes•77 views

A handout I formulated to bolster nursing education during an internship/Advanced Pharmacy Practice Experience (APPE) in medication safety at a hospital.

Recommended
More Related Content
Similar to Nursing Education: Appetite Stimulants for Elderly Patients
Similar to Nursing Education: Appetite Stimulants for Elderly Patients (20)
More from Paul Pasco
More from Paul Pasco (17)
Recently uploaded
Recently uploaded (20)
Nursing Education: Appetite Stimulants for Elderly Patients
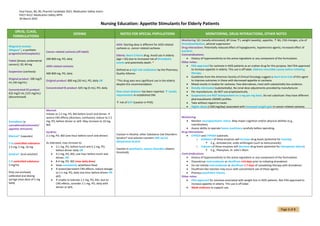
- 1. Paul Pasco, BA, BS, PharmD Candidate 2022, Medication Safety Intern PHCY 4522: Medication Safety APPE 30 March 2022 Page 1 of 3 Nursing Education: Appetite Stimulants for Elderly Patients DRUG, CLASS, FORMULATIONS DOSING NOTES FOR SPECIAL POPULATIONS MONITORING, DRUG INTERACTIONS, OTHER NOTES Megestrol acetate (Megace®), a synthetic progestin/antineoplastic) Tablet (breast, endometrial cancers): 20, 40 mg Suspension (cachexia): Original product: 200 mg/5 mL (40 mg/mL) Concentrated ES product: 625 mg/5 mL (125 mg/mL) (discontinued) Cancer-related cachexia (off-label): 200-800 mg, PO, daily AIDS-related cachexia: 400-800 mg, PO, daily Original product: 800 mg (20 mL), PO, daily OR Concentrated ES product: 625 mg (5 mL), PO, daily AIDS: Starting dose is different for AIDS-related cachexia vs. cancer-related cachexia. Elderly: Beers Criteria drug. Avoid use in elderly (age > 65) due to increased risk of thrombotic events and potentially death. * Defined as a high-risk medication by the Pharmacy Quality Alliance. *This drug sees very significant use in the elderly despite this recommendation. New-onset diabetes has been reported. ↑ insulin requirements in established DM. ↑ risk of DVT (caution in PVD). Monitoring: SCr (renally eliminated), BP (may ↑), weight (weekly), appetite, ↑ BG, CNS changes, s/sx of thromboembolism, adrenal suppression Drug interactions: Potentially reduced effect of hypoglycemic, hypotensive agents; increased effect of warfarin. Contraindications: • History of hypersensitivity to the active ingredient or any component of the formulation. Other notes: • FDA-approved for cachexia in AIDS patients as an orphan drug for this purpose. Not FDA-approved to increase appetite in elderly. This use is off-label. Address reversible causes before initiating therapy. • Guidelines from the American Society of Clinical Oncology suggest a short-term trial of this agent to improve outcomes in those with decreased appetite or cachexia. • Mixed results in studies for cachexia. Few alternatives, most with substantially less evidence. • Renally eliminated (substantially). No renal dose adjustments provided by manufacturer. • Per manufacturer, do NOT use prophylactically. • Suspensions are NOT bioequivalent on a mg-per-mg basis. Do not substitute: they have different pharmacokinetic (ADME) profiles. • Take without regard to meals. • Higher doses (>160 mg/day) associated with increased weight gain in cancer-related cachexia. Dronabinol (a cannabinoid/antiemetic/ appetite stimulant) Marinol® (capsules) C-III controlled substance 2.5 mg, 5 mg, 10 mg Syndros® (oral solution) C-II controlled substance 5 mg/mL Only use enclosed, calibrated oral dosing syringe (max dose of 5 mg held) Marinol: Initiate at 2.5 mg, PO, BID before lunch and dinner. If severe CNS effects (dizziness, confusion), reduce to 2.5 mg, PO, before dinner or qHS. May increase to 10 mg, BID. Syndros: 2.1 mg, PO, BID (one hour before lunch and dinner) As tolerated, may increase to: • 2.1 mg, PO, before lunch and 4.2 mg, PO, before dinner daily OR • 4.2 mg, PO, BID, one hour before lunch and dinner, OR • 8.4 mg, PO, BID (max daily dose) • Dose consistently w/without food. • If severe/persistent CNS effects, reduce dosage to 2.1 mg, PO, daily one hour before dinner OR qHS. • If unable to tolerate 2.1 mg, PO, BID, due to CNS effects, consider 2.1 mg, PO, daily with dinner or qHS. Caution in Alcohol, other Substance Use Disorders: Syndros® oral solution contains 50% (w/w) dehydrated alcohol Caution in psychiatric, seizure disorders (lowers threshold) Monitoring: • Monitor neuropsychiatric status. May impair cognition and/or physical abilities (e.g., coordination). • Assess ability to operate heavy machinery carefully before operating. Drug interactions: • CYP2C9 and CYP3A4 substrate. o Inhibitors of these enzymes will increase drug levels (potential for toxicity). ▪ E.g., Amiodarone, azole antifungals (such as ketoconazole). o Inducers of these enzymes will decrease drug levels (potential for therapeutic failure). ▪ E.g., Phenytoin, St. John’s Wort. Contraindications: • History of hypersensitivity to the active ingredient or any component of the formulation. • Discontinue metronidazole or disulfiram ≥14-days prior to initiating dronabinol. • Do not initiate metronidazole or disulfiram ≤ 7-days of completing therapy with dronabinol. • Disulfiram-like reaction may occur with concomitant use of these agents. • Previous psychiatric history. Other notes: • FDA-approved for anorexia associated with weight loss in AIDS patients. Not FDA-approved to increase appetite in elderly. This use is off-label. • Weak evidence to support use.
- 2. Paul Pasco, BA, BS, PharmD Candidate 2022, Medication Safety Intern PHCY 4522: Medication Safety APPE 30 March 2022 Page 2 of 3 Cyproheptadine (Periactin®), an H1RA, 5-HT2 antagonist 4 mg tablets 2 mg, PO, four times daily for 1 week, then 4 mg, PO, four times daily Elderly: Beers Criteria drug. Avoid use in elderly (age > 65) due to anticholinergic properties (can cause confusion). Monitoring: • Monitor neuropsychiatric status. May impair cognition and/or physical abilities (e.g., coordination). • Assess ability to operate heavy machinery carefully before operating. Drug interactions: • MAOI therapy (↑ anticholinergic effects and duration). • ↑ sedation with other sedatives (alcohol, hypnotics, tranquilizers, etc.) Contraindications: • History of hypersensitivity to the active ingredient or any component of the formulation. • MAOI therapy. Other notes: • Completely off-label use. Not FDA-approved for appetite stimulation in ANY population. • Not FDA-approved to increase appetite in elderly. This use is off-label. Oxandrolone (Oxandrin®, brand discontinued), synthetic, anabolic, androgenic steroid C-III controlled substance, 2.5 mg, 10 mg tablets 2.5 mg to 20 mg, PO, in two to four divided doses for 2-4 weeks and repeated PRN Males with prostate cancer: Do not use. Females (risk for hirsutism): Caution (risk vs. benefit) Persons with hyperlipidemia: Caution (risk vs. benefit) Monitoring: • ↑ LFTs (jaundice, hepatitis), Ca2+ levels (hypercalcemia), ↑ PSA (increased risk for prostate carcinoma), ↑ appetite, ↑ weight, ↑ lipid profile (potential for ↑LDL and ↓HDL), ↑ virilization in women (e.g., hirsutism) Drug interactions: • Concomitant administration of oxandrolone and warfarin may ↑↑↑ INR. May require ↓↓↓ oxandrolone doses to prevent. Contraindications: • History of hypersensitivity to the active ingredient or any component of the formulation. • Known or suspected carcinoma of the male breast or prostate. • Carcinoma of the female breast with hypercalcemia. • Nephrosis. • Hypercalcemia. Other notes: • FDA-approved as adjunctive therapy to mitigate muscle wasting secondary to long-term use of glucocorticosteroids • Not FDA-approved to increase appetite in elderly. This use is off-label. • Inhibits clotting factors VII, V, X, and II (similar to warfarin). Dexamethasone (Decadron®), glucocorticosteroid 0.5 mg, 0.75 mg tablets Other agents in this class may be substituted. 3-4 mg dexamethasone (or equivalent) for a few weeks and then readjusted based on risk assessment. Caution in: T1DM, T2DM, postmenopausal women, elderly, psychiatric diagnoses (e.g., Intermittent Explosive Disorder) Monitoring: • Glucose (hyperglycemia), bone mineral density (osteoporosis with long-term use), mental status changes (irritability/agitation/mood swings), WBC with CBC (leukocytosis), ↑ weight, ↑ appetite Drug interactions: • ↓ effectiveness of hypoglycemic agents. • Inducer of CYP3A4/5 and P-gp ➔ ↓ concentration of substrate drugs (e.g., atorvastatin, simvastatin). • ↓ efficacy of vaccinations. Contraindications: • History of hypersensitivity to the active ingredient or any component of the formulation. • Systemic fungal infections. Other notes: • Effective at increasing appetite but very significant side effect profile. • Not FDA-approved to increase appetite in any populations. This use is off-label.
- 3. Paul Pasco, BA, BS, PharmD Candidate 2022, Medication Safety Intern PHCY 4522: Medication Safety APPE 30 March 2022 Page 3 of 3 Mirtazapine (Remeron®), tetracyclic, atypical antidepressant (antagonist of 5-HT2, 3 receptors) 15, 30, 45 mg tablets 15-30 mg, PO, daily BBW for ↑ suicidality in pediatric and young adult patients. Elderly: Beers Criteria drug. Avoid use in elderly (age > 65) due to potential for orthostasis/falls. Monitoring: • Mood (suicidality), sedation, CBC (agranulocytosis; rare but serious) Drug interactions: • CYP2D6, 3A4/5, 1A2 inducers: ↓ drug levels, ↓ efficacy (and potentially therapeutic failure) • CYP2D6, 3A4/5, 1A2 inhibitors: ↑ drug levels, ↑ efficacy (and potentially toxicity) Contraindications: • History of hypersensitivity to the active ingredient or any component of the formulation. • Use of an MAOI <14 days prior to discontinuing mirtazapine. • Use of mirtazapine <14 days prior to discontinuing an MAOI. Other notes: • Not FDA-approved to increase appetite in any populations. This use is off label. • ~50% renally eliminated. Use caution in renal impairment and adjust dose if needed. Sources: 1. Journal of the National Cancer Institute. Controlled Trial of Megestrol Acetate for the Treatment of Cancer Anorexia and Cachexia. Journal of the National Cancer Institute (JNCI). Published July 4, 1990. Accessed March 30, 2022. https://academic.oup.com/jnci/article-abstract/82/13/1127/970754?redirectedFrom=fulltext&login=false 2. Bristol-Myers Squibb Company. Megace® (Megestrol Acetate, USP) Oral Suspension. Bristol-Myers Squibb Company; 2012:1-13. Accessed March 28, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020264s017lbl.pdf 3. Benuvia Therapeutics Inc. Highlights of Prescribing Information: Syndros® (Dronabinol).; 2020:1-21. Accessed March 30, 2022. https://syndros.com/wp-content/uploads/2021/04/Syndros-Package-Insert-2021-1.pdf 4. Solvay Pharmaceuticals, Inc. Marinol® (Dronabinol) Capsules. Solvay Pharmaceuticals, Inc; 2006:1-11. Accessed March 30, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2006/018651s025s026lbl.pdf?msclkid=6512a127b03f11ec9b1e4b20b32976c5 5. Homnick DN, Marks JH, Hare KL, Bonnema SK. Long‐Term Trial of Cyproheptadine as an Appetite Stimulant in Cystic Fibrosis. Pediatric Pulmonology. 2005;40(3):251-256. doi:10.1002/ppul.20265 6. Sandoz Inc. Oxandrolone Tablets USP. Sandoz Inc.; 2006:1-2. Accessed March 30, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2006/076897lbl.pdf?msclkid=5fde46d6b05511ec8a6f1a93341a7627 7. Roeland EJ, Bohlke K, Baracos VE, et al. Management of Cancer Cachexia: ASCO Guideline. American Society of Clinical Oncology Journal. 2020;38(21):2438-2453. doi:10.1200/jco.20.00611 8. Merck & Co., Inc. DECADRON ® (DEXAMETHASONE TABLETS, USP). Merck & Co., Inc.;1-8. Accessed March 30, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2004/11664slr062_decadron_lbl.pdf?msclkid=4e792f4db05c11eca9b2389262f3c485 9. Organon USA Inc. Remeron (mirtazapine) Tablets. Fda.gov. Published May 2007. Accessed March 30, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2007/020415s019 10. Riechelmann RP, Burman D, Tannock IF, Rodin G, Zimmermann C. Phase II Trial of Mirtazapine for Cancer-Related Cachexia and Anorexia. American Journal of Hospice and Palliative Medicine®. 2009;27(2):106-110. doi:10.1177/1049909109345685