
Recommended
More Related Content
What's hot
What's hot (20)
Similar to ACCURATELY ESTIMATING BLOOD LOSS
Similar to ACCURATELY ESTIMATING BLOOD LOSS (20)
More from Nisar Arain
More from Nisar Arain (20)
Recently uploaded
Recently uploaded (20)
ACCURATELY ESTIMATING BLOOD LOSS
- 1. -BLOOD ESTIMATION -Dr Nisar Ahmed Arain Assistant Professor Anesthesia/Critical Care/ER
- 2. VISUAL INSPECTION -It is Inaccurate. In some reports, the amount of blood estimated to have been lost by inspection was half the measured loss CLINICIANS -They typically under estimate Post-Partum blood loss by 30% to 40% IMPORTANTLY -In Obstetrics, part or all of the hemorrhage may be concealed -Clinicians commonly record blood loss using inaccurately low numbers “How can we teach people to accurately and honestly record blood loss
- 3. ON AVERAGE -Women lose about a- 500 ml in a b-1000 ml in CS C-1500 ml in a cesarean Hysterectomy. THE CRITICAL AREA -Where you want to estimate blood loss is over 2,000 ml, and we almost always underestimate that. By that point, the patient has Hypotension, and has significant tachycardia, and is in SHOCK
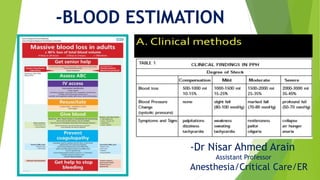
- 4. -Clinical Methods of Estimation
- 5. -Blood Pressure and Heart Rate --By the time you detect changes in Blood pressure OR Heart rate suggesting PPH, the women already has lost 1/3rd of her blood volume --Orthostatic Hypotension would tell you that patient has lost 20% to 25% of her blood, but if she is sitting or lying down on the delivery table, you are unlikely to detect that symptom. --Hypotension reflects a loss of 30% to 35% of blood volume. “Do not wait for Hypotension to develop along with its signs and symptoms” and to treat for PPH “Do not wait to start seeing S and S. -1-Blood Pressure and Heart Rate
- 6. -Hematocrit --It needs 4 hours for significant changes and 48 hours for complete compensation --In acute hemorrhage, the immediate Hematocrit may not reflect acute blood loss --After the loss 1000 ml of blood, the hematocrit typically falls only 3 volume percent in the first hour --When resuscitation is given with rapid infusion of I/V crystalloids, there is a rapid equilibrium in the circulation. --During an episode of acute significant hemorrhage, the initial hematocrit is always in the highest limits. This is true weather it is measured in the delivery room or operation room, or recovery room. -2--Hematocrit
- 7. --Urine output --One of the most important “vital signs” to follow in the bleeding patient with obstetrical Hemorrhage. --In the absence of Diuretics, the rate of urine formation reflects the adequacy of renal perfusion and, in tern, perfusion of other vital organs, because renal blood flow is especially sensitive to the changes in the blood volume. --Urine flow of atleast 30 ml and preferably 60 ml per hour should be maintained --With potentially serious hemorrhage, an indwelling catheter should be inserted to measure urine flow. -3-Urine output
- 8. --4-Weighing Packs:- and correlate with blood loss: Hospitals keeps scales in the Delivery rooms to weigh Lap sponges and other materials to estimate blood loss 1 kg soaked swabs = 1000 ml -5-perhaps the easiest method of estimating is to picture a soda can which would hold about 350 ml of blood. When you look at blood clots or blood in a canister, estimate how many cans of soda are represented and you will be close to blood volume lost. The principal is to recognize volume
- 9. 6- Maximum Capacity of Swabs a-Small =(10 X 10 cm) 60 ml b-Medium =(30 X30 cm) 140 ml c-Large =(45 X 45 cm) 350 ml 7-Floor Spill a-50 cm Diameter = 500 ml b-75 cm Diameter = 1000 ml c-100 cm Diameter = 1500 ml 8-Vaginal PPH Limited to bed only:- Unlikely to exceed 1000 ml Spilling from bed to Floor likely to exceed 1000 ml
- 10. -B-Actual Blood Loss --In the Perioperative period clinical estimation of blood loss is inaccurate and alone should not be used to determine the need for red blood cells transfusion --Poor agreement between the actual blood loss and the estimated blood loss. The 95% confidence intervals (-719.939 ml to 1265.619 ml) suggest that clinical estimation alone may result in unacceptable under or over transfusions --In 64%of the cases the blood loss was under estimated. --Clinical estimation of blood loss suffer from large interobserver variability and poor repeatability.
- 11. --The extent of blood loss and response to transfusion is reflected in the changes in the Hematocrit --This change may be used to calculate the actual blood loss using suitable formulae -Actual Blood Loss cont.
- 12. -Actual Blood Loss --It is a modification of the gross formula ABL = BV [Hct (i) – Hct (f) / Hct (m) BLOOD VOLUME = Body weight in Kgms X 70 ml Kg – 1 Hct (i), Hct (f) and Hct (m): the initial, final and mean (of the initial and final) Hematocrits respectively BLOOD VOLUME a-NEONATES = 85 to 90 ml / Kg body weight b-CHILDREN = 80 ML / Kg body weight c-ADULTS = 70 ml / Kg body weight
- 13. -Calculating blood loss in theatre --1-Weigh a Dry Swab --2-Weigh blood soaked swabs as soon as they are discarded and subtract their dry weight (1 ml of blood weighs approximately 1 gm) --3-Substract the weight of empty “suction bottles” from the filled ones --4-Estimate blood loss into surgical drapes, together with the pooled blood beneath the patient and onto the floor. --5-Note the Volume of irrigation fluids, subtract this volume from the measured blood loss to estimate the final blood loss
- 14. -The Decision to transfuse Blood -Percentage Method -Calculate the patients blood volume -Decide on the percentage of blood volume that could be lost but safely tolerated, depending on the clinical condition of the patient, provided that Normovolemia is maintained
- 15. Patient condition Health Average Poor Patient condition Health Average Poor Percentage method Acceptable loss of blood volume before transfusion method 30% 20% <10% Haemodilution Hb 7-8g/dl Hct 21-24% 8- 9g/dl 24-27% 10g/dl 30%
- 16. -HEMODILUTION METHOD --Decide on the lowest acceptable Hb or Hematocrit (Hct) that may be safely tolerated by the patient --Calculate the allowable volume of blood loss that can occur before a blood transfusion becomes necessary. --Replace the blood loss up to the allowable volume with Crystalloid or colloid fluids to maintain Normovolemia. --If the allowable blood loss volume is exceeded, further replacement should be with blood
- 17. --Which ever method is used, the decision to transfuse will depend on the clinical condition of the patient and supply. This particularly limited in patients with evidence of severe cardiac or respiratory disease or pre-existing anemia --The methods described are simple guidelines which must be altered according to the clinical situation. --Further blood loss should be anticipated, particularly postoperatively --Whenever possible, transfuse blood when surgical bleeding is controlled. This will maximize the benefits of the transfusion
- 18. --The American college of Physicians recommended that RBC transfusions should be done Unit by Unit and the patient should be evaluated between each transfusion. --Excessive intraoperative transfusion and the practice of administering blood without Re-Evaluating the Hematocrit in between resulted in 90% of the un-necessary transfusions --Determination of the Hematocrit immediately before administration of each unit would reduce blood consumption by 25%.
- 19. -STRONG RECOMENDATIONS -A PROGRAM TO TRAIN DOCTERS AND NURSES TO ESTIMATE BLOOD LOSS PERFACTLY IS RECOMENDED
- 20. THANK YOU