In-field gait retraining reduces impact forces in runners with tibial stress injuries
1. Participants experienced a 21% reduction in impact forces at MOD
which were maintained with the “Go, No-Go” dual task.
However, there was a 17.8% increase in dual task latency with the
modified gait pattern.
After in-field gait retraining was completed, the reductions in impact
forces remained.
Importantly, performance on the “Go, No-Go” dual task returned to
baseline levels suggesting that skill consolidation occurred.
Runners likely reduced impact forces by reducing vertical
oscillation.
Reductions in impact forces that were noted after the in-field gait
retraining were consistent with a previous study using the same
technique in healthy runners.5
Increased SR previously suggested to reduce risk of tibial stress
fracture in a probabilistic model.6
Data suggest only modest inc. in SR needed to reduce loading in
runners with previous history of tibial stress injuries
Further, our data indicate that a reduction in dual task ability can be
expected during the skill acquisition stage of motor learning.
Can be easily adopted in practice: Garmin feedback computer
costs ~$120. In-field program reduces need for clinic visits.
1. Ross & Allsopp. Mil Med. 2002;167:560-5.
2. Tenforde et al. Med Sci Sports Exerc. 2013;45: 1843-51.
3. Zadpoor AA Nikooyan A. Clin Biomech. 2011;26(1):23-28.
4. Milner CE et al., Med Sci Sports Exerc. 2014;46(5):973-981
5. Willy RW et al., Scand. J. Med. Sci & Sp. 2016; 26(2)” 197-205
6. Edwards WB et al. Med Sci Sports Exerc. 2009;41(12):2177-84.
Tibial stress injuries are particularly disabling, requiring enforced rest for
4-17 weeks and result in medical discharge in 39%-60% of military
Cadets.1
Runners with a past history of TSI have a six-fold increase in risk of
sustaining a subsequent TSI.2
Excessive impact forces during running are related to tibial stress
fractures.3,4
In-field feedback on SR is effective at reducing impact forces during
running by 18% in healthy individuals.5
Unknown if in-field gait retraining will yield similar outcomes in runners
with a history of tibial stress injury.
Additionally, gait retraining may result in a reduced ability to perform
dual tasks, which are necessary during military operations.
We sought to determine the effectiveness of an in-field gait retraining
program in runners with a recent history of tibial stress injury. A
secondary purpose was to determine if this program would have a
detrimental effect on dual task performance
INTRODUCTION
METHODS
To date, 7 runners have completed the retraining protocol. (Table 1)
In order to qualify for this study, participants were required to be running
at least 8 miles per week and have a recent (within 4 years) history of
tibial stress injury.
Baseline: All participants attended a baseline data collection. Baseline
running mechanics were collected while participants completed a “Go,
No-Go” task.
Next, participants were issued an accelerometer-based running
computer (Figure 1, Garmin, Olathe, KS).
Gait Modification: Runners were instructed to increase their running
cadence by 5-10%, in response to feedback from running computer
(Figure 1). Running mechanics were again sampled and “Go, No-Go”
performance was assessed.
Figure 1: 1a) a wireless accelerometer transmitted data to the wrist mounted
running computer. 1b) the wrist mounted running computer was configured such
that running duration, real time strides per minute (steps per minute/2), alarm
sounded when spm was out of range of 5-10% 1c) During mobile monitoring period
subjects were unable to view spm.
Retraining Phase: 8 sessions of band width feedback on step rate, via
the running computer, during in-field running. Instructed to maintain inc.
SR by 5-10%.
Post-retraining: Running mechanics and “Go, No-Go” performance were
reassessed.
Preliminary analysis performed with effect sizes (Cohen’s d).
Ongoing study. We aim to finish data collections in May 2016.
Long term follow-up and randomized control trial needed to
determine if an increase in step rate reduces reoccurrence of tibial
stress injuries in this cohort.
Cognitive performance during a gait retraining program to address running mechanics associated
with tibial stress injuries
Niland S2, Murray N2, Baggaley M1, Meardon S1, Willson JD1,Willy RW1
1Department of Physical Therapy, East Carolina University, 2Department of Kinesiology, East Carolina University
RESULTS
REFERENCES
LIMITATIONS
CLINICAL RELEVANCE
DISCUSSION
Figures 2-4: 2. 3D analysis of running on split belt treadmill 3. “Go, No-Go” task 4. Analysis of gait
mechanics during instrumented treadmill running.
Fig. 2
Fig 2
Demographics Mean (sd)
Age (years) 20.1 (1.2)
BMI(kg/m2) 23.7 (3.3)
Weekly running volume (km per week) 19.8 (7.4)
Self-selected pace (m/sec) 2.8 (0.2)
Running experience (years) 6.6 (2.0)
Treadmill comfort (x/10) 9.7 (0.8)
Males/Females (n) 1/6
Work funded by East Carolina University Interdisciplinary Grant.
Michele Hudgins, Caitlin Melton, Tyler Whittier and Barbara Cherry
assisted with data collections.
ACKNOWLEDGEMENTS
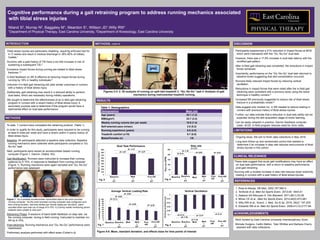
Figure 5-8: Mean, standard deviation, and effects sizes for time points of interest
METHODS, CONT’D
Table 1: Demographics
d= -1.31
d= -2.27d= 1.57
Mod
Fig. 5
d= 1.16
d= 0.14
d= 0.08
d= 2.27
d= -0.02
ModMod
Fig. 6
d= -0.63
d= -0.13
d= -0.09
d= -0.82
d= -0.36
ModMod
Fig. 7
d= 1.78
d= 0.13 d= 0.15
d= -0.37
ModMod
Fig. 8
d= 3.16
Fig. 2 Fig. 3 Fig. 4
These data suggest that acute gait modifications may have an effect
on dual task performance, with a return to baseline performance
post-gait retraining.
Running with a modest increase in step rate reduces lower extremity
loading in runners with a past history of tibial stress injuries.