Arming the Rapid Response Team with Intraosseous Needles Reduces Time to First Medication and Improves Post-Code Survival to ICU Transfer
•
1 like•255 views

Dana Goforth, RN, BSN; Dan Lantos, RN, MSN, CNML; Nick Leary, RN, BSN, PCCN, CCRN; Cindy Brenton, RN, MSN, NEA-BC.
Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (12)
Similar to Arming the Rapid Response Team with Intraosseous Needles Reduces Time to First Medication and Improves Post-Code Survival to ICU Transfer
Similar to Arming the Rapid Response Team with Intraosseous Needles Reduces Time to First Medication and Improves Post-Code Survival to ICU Transfer (20)
Recently uploaded
Recently uploaded (20)
Arming the Rapid Response Team with Intraosseous Needles Reduces Time to First Medication and Improves Post-Code Survival to ICU Transfer
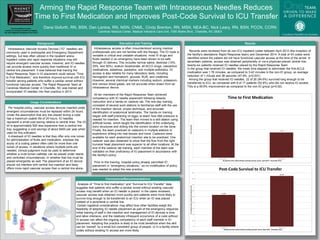
- 1. Arming the Rapid Response Team with Intraosseous Needles Reduces Time to First Medication and Improves Post-Code Survival to ICU Transfer Carolinas Medical Center, a facility of Carolinas HealthCare System, has been Magnet® designated since 2013 Dana Goforth, RN, BSN, Dan Lantos, RN, MSN, CNML, Cindy Brenton, RN, MSN, NEA-BC, Nick Leary, RN, BSN, PCCN, CCRN Carolinas Medical Center, Medical Intensive Care Unit, 1000 Blythe Blvd., Charlotte, NC 28203 Background Intraosseous Vascular Access Devices (“IO” needles) are commonly used in prehospital and Emergency Department settings, but less often utilized in the inpatient arena. Inpatient codes and rapid response situations may still require emergent vascular access, however, and IO needles can provide access more quickly than traditional IV or central line placement. It was believed that training the Rapid Response Team in IO placement could reduce “Time to First Medication,” and therefore improve survival until ICU transfer among patients who suffer a cardiac arrest without functional vascular access. The Rapid Response Team at Carolinas Medical Center in Charlotte, NC was trained and incorporated IO needles into their practice in 2013. Intraosseous access is often misunderstood among medical professionals who are not familiar with the therapy. The IO route is versatile in critical and unstable situations: most IV drugs and fluids needed in an emergency have been shown to be safe through IO delivery. This includes normal saline, dextrose (10%, 25%, and 50%), sodium bicarbonate, all ACLS drugs, vasoactive medications, sedatives, paralytics, and multiple antibiotics. IO access is also reliable for many laboratory tests, including hemoglobin and hematocrit, glucose, BUN, and creatinine. However, several chemical markers including sodium, potassium, and venous blood gases, are not accurate when drawn from an intraosseous device. All ten members of the Rapid Response Team achieved competency with IO needle placement following didactic instruction and a hands-on cadaver lab. The one-day training consisted of several work stations to familiarize staff with the use of the insertion device, proper technique, and accurate identification of anatomical landmarks. The hands-on training began with staff practicing on eggs, to teach how little pressure is needed for insertion. The team then moved to a skill station using artificial bones, which taught the identification of the underlying bony structures and drilling into the correct location on the bone. Finally, the team practiced on cadavers in multiple stations to experience drilling into real tissues and bone. Cadavers were available for each anatomical insertion site to be practiced. One cadaver was also dissected to show that the flow from the right humeral head placement was superior to all other locations. At the end of the cadaver lab training, each member of the team was validated on their proficiency of IO placement in accordance with the facility's policy. Prior to this training, hospital policy already permitted IO placement in “emergency situations,” so no modification of policy was needed to adopt the new practice. Education and Training Usage Considerations Per hospital policy, vascular access devices inserted under emergent circumstances must be replaced within 24 hours. Under the assumption that any line placed during a code has a maximum usable life of 24 hours, IO needles represent a small cost saving relative to central lines. The IO kit is approximately $20 less expensive than a central line tray, suggesting a cost savings of about $400 per year when used for this indication. A drawback of IO needles is that they offer only one lumen for administration of fluids and medication, whereas the acuity of a coding patient often calls for more than one lumen of access. In situations where multiple ports are needed, clinical judgment must be used to determine whether a multi-lumen catheter can be placed under sterile and controlled circumstances, or whether that line must be placed emergently as well. The placement of an IO device should not interfere with central line insertion and likely offers more rapid vascular access than a central line alone. Results Conclusions/Recommendations Analysis of “Time to first medication” and “Survival to ICU Transfer” data suggests that patients who suffer a cardiac arrest without existing vascular access may benefit when an IO needle is placed. In the cases reviewed, vascular access was obtained more quickly and patients were more likely to survive long enough to be transferred to an ICU when an IO was placed instead of a peripheral or central line. Certain logistical considerations may affect how other facilities weigh the feasibility of adopting IO needle placement as part of the emergency response. Initial training of staff in the insertion and management of IO devices is time and labor-intensive, and the relatively infrequent occurrence of a code without IV access can affect the ongoing competency of each staff member in IO placement. Adopting this practice is likely to be most beneficial when the skill can be “owned” by a small but consistent group of people, or in a facility where codes without existing IV access are more likely. N=26 3.42 1.78 0 1 2 3 4 No IO placed (N=17) IO placed (N=26) Time(minutes) All patients who coded without working vascular access, April 2013 - December 2014 Time to First Medication 52.9% 84.6% 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% No IO placed (N=17) IO placed (N=26) %ofpatientswhosurviveduntiltransfertoICU All patients who coded without working vascular access, April 2013 - December 2014 Post-Code Survival to ICU Transfer Records were reviewed from all non-ICU inpatient codes between April 2013 (the inception of the facility’s standalone Rapid Response team) and December 2014. A total of 43 codes were identified where the patient did not have functional vascular access at the time of the arrest. In seventeen patients, access was obtained peripherally or via a physician-placed central line; twenty-six patients received IO needles placed by the Rapid Response Team. In the group that received IO needles, the mean time elapsed to administer the first ACLS medication was 1.78 minutes, as compared to 3.42 minutes in the non-IO group, an average reduction of 1 minute and 38 seconds (47.9%, p<0.001). Among the group that received IO needles, 22 of 26 (84.6%) survived long enough to be transferred to ICU, as compared with 9 of 17 patients (52.9%) who did not receive IO access. This is a 59.9% improvement as compared to the non-IO group (p=0.02). http://www.teleflex.com/en/usa/ezioeducation/index.html