Calciphylaxis
•Download as PPTX, PDF•
0 likes•565 views

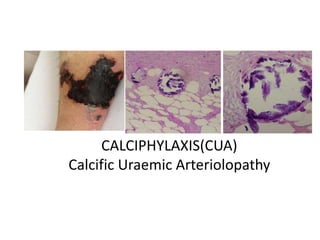
Calciphylaxis, also known as calcific uremic arteriolopathy, is a rare disorder characterized by calcification of the small blood vessels of the skin and subcutaneous fat. It most commonly occurs in patients with end-stage renal disease on dialysis. The calcification leads to reduced blood flow and painful skin lesions. Risk factors include hyperparathyroidism, vitamin D use, and warfarin use. Diagnosis is made clinically and confirmed with biopsy showing vessel calcification. Treatment involves sodium thiosulfate, hyperbaric oxygen, bisphosphonates, and wound care. Prognosis is poor with high mortality rates due to complications like infection and organ failure.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Calciphylaxis
Similar to Calciphylaxis (20)
More from Naveen Kumar
More from Naveen Kumar (17)
Recently uploaded
Recently uploaded (20)
Calciphylaxis
- 1. CALCIPHYLAXIS(CUA) Calcific Uraemic Arteriolopathy ADD SOME RELATED PICTURE
- 2. OUTLINES • INTRODUCTION • PATHOGENESIS • EPIDEMIOLOGY • RISK FACTORS • NON ESRD POPULATION • CLINICALFEATURES • DIAGNOSIS AND DD • LAB MANIF/BIOPSY/ RADIOLOGY • TREATMENT • OUTCOME
- 3. CALCIFIC URAEMIC ARTERIOLOPATHY Introduction • CUA or calciphylaxis is a rare disorder (Orphan disease)of microvascular occlusionof subcutaneous adipose tissue & dermis leading to painful skin lesions- Calciphylaxis Cutis /Visceral Calciphylaxis. • Associated histologically with media calcification of small & medium-size vessels in dermis & subcutaneous adipose tissue • Has an estimated incidence of <1% among dialysis patients who are predominantly affected cohort
- 5. EPIDEMIOLOGY-RELEVANCE • Calciphylaxis most commonly occurs in patients of ESRD and are on dialysis but may also occur in kidney tx recipients & in non-ESRD patients • Is a lethal disease with an estimated six-month survival of approx 50% with no approved RX
- 8. NON UREMIC CALCIPHLAXIS 60% had been previously treated with glucocorticoids, and 25% with warfarin •Nigwekar SU, Wolf M, Sterns RH, Hix JK. Calciphylaxis from nonuremic causes: a systematic review. Clin J Am Soc Nephrol 2008; 3:1139.
- 11. Severe sec HPT /vascular calcif
- 12. PATHOGENESIS Calciphylaxis is a poorly understood disorder. The skin lesions of calciphylaxis result from reductions in the arteriolar blood flow. Reduced blood flow is caused by calcification, fibrosis, and thrombus formation primarily involving the dermo-hypodermic arterioles Hyperparathyroidism, deficiencies in inhibitors of vascular calcification, and chronic inflammation have also been implicated in the pathogenesis of calciphylaxis
- 13. PATOGENESIS • Microvascular calcification occurs first likely via an active process involving up regulation of factors involved in osteogenesis and bone remodeling, including bone morphogenetic protein 2 (BMP-2), runt-related transcription factor 2 (RUNX-2) and osteopontin • Adipocytes may also play an important role in the development of vascular calcification of calciphylaxis . • Ongoing vascular endothelial injury causes cutaneous arteriolar narrowing and thrombosis leading to tissue infarction
- 14. PATHOGENETIC FACTORS • Factors presumed to be involved in the widespread calcification are - Chronic kidney disease-mineral bone disorder (CKD- MBD) and its treatment (including hyper parathyroidism, abnormalities in calcium and phosphate, and vitamin D administration) - Deficiencies of the inhibitors of vascular calcifications and chronic inflammation
- 17. Clinical recognition • Typical sites- high fat tissue area • Typical appearance – early red to violet/later black • Typical symptom- extremely painful • Typical risk factors- esrd/warfarin/ autoimm • Atypical sites need DD
- 18. What do we see and where? Time of presentation – Early -late. • Mottled skin (livedo reticularis)- Violaceous/red • Purpuric plaque-like subcutaneous nodules, indurations • Bullae over plaque ,Necrotic ulcers with eschars (skin/subcutaneous fat/ muscle) • Typical lesions seen more in central body area than on finger and toes (areas with high adipose tissue content)
- 19. Followed the path of the vasculature Intense pain is a constant finding
- 21. Digital gangrene in a dialysis patient due to calciphylaxis and systemic polyarteritis nodosa: A diagnostic dilemma Jain N; Sethi J; Ramachandran R; Kumar V; Rathi,M, et al. Ind J of Nephrology 2019 Left foot gangrenous changes and redness swelling of all toes with ulcer on dorsal aspect
- 23. Differential diagnosis Many dermatologic conditions resemble the superficial lesions of Calciphylaxis Diagnosis Distinguishing characteristic(s) Antiphospholipid syndrome Serum antiphospholipid antibodies Radiation arteritis Radiation arteritis Vasculitis Significant inflammatory infiltrate Dystrophic calcification Localized tissue damage secondary to calcium and phosphorous deposition; normal serum calcium and phosphorous levels Cholesterol emboli Acute onset; biopsy shows cholesterol crystals embedded within intramural thrombi; lesions distributed in extremities with acral involvement
- 24. Differential diagnosis Diagnosis Distinguishing characteristic(s) Panniculitis Biopsy reveals inflammatory infiltrate in the adipose tissue without calcification of vessels Purpura fulminans Sepsis and disseminated intravascular coagulation often present; increased partial thromboplastin time, prothrombin time, fibrinogen, D-dimers Warfarin necrosis History of warfarin use Heparin necrosis History of heparin use; occurs uniquely at sites of intramuscular heparin injection Atherosclerosis obliterans Affects intimal layer of the abdominal aorta and small- to medium-sized arteries in the lower extremities, often resulting in elimination of the popliteal, posterior tibial, and/or dorsalis pedis pulses
- 25. Histological features on Biopsy • Calcification of medial wall of arterioles dermo- hypodermal and pannicular region • Intimal proliferation & fibrosis, endovascular thrombosis • Ischaemic pathology distal to vessels
- 26. Role of Imaging in diagnosis • Plain X Ray/3D CT/ Mammography-limited role Demonstrates an arborisation of vascular calcification within the dermis and the subcutaneous tissue &numerous echogenic foci suggestive of large calcifications-best detected by mammoographic technique or CT reconstruction rather than plain xray • BONE SCAN OR SCINTIGRAPHY Three-phase technetium 99m methylene diphosphate bone scan to identify cutaneous calcifications
- 27. Role of Imaging in diagnosis • X-ray : Detects vascular calcification within the dermis and subcutis - “ Net-like” - Mammography film better detects small vessels • Bone scintigraphy : -Scans entire body -Detects micro calcificatio of soft tissue -Evaluates extent of disease and response to treatment -89% sensitivity,97% specificity
- 29. Bone scintigraphy Demonstrate bone matrix protein osteopontin
- 31. Treatment of Calciphylaxis • Optimising dialysis adequacy • Sodium thiosulfate (off-label use) • PD to HD transition • Hyperbaric oxygen therapy • Bisphosphonates
- 32. Sodium Thiosulphate • Currently, the first-line treatment of calciphylaxis without secondary HPT • It is a potent antioxidant and it also increases the solubility of calcium deposits • It causes rapid pain relief and successful wound healing within weeks to months of initiating therapy • Median-duration-96days(median-no38days)in literature
- 33. Dose • Dose: 25 g iv 3 times per week following dialysis • Infusion times vary from 30-60 minutes in last h of hd • Reduce the dose of STS to 12.5 g for patients weighing <60 kg and those weighing ≥60 kg who cannot tolerate the higher dose. One should stop STS in patients who fail to respond to STS within the first two to four weeks.
- 34. Hyperbaric oxygen • Breathing 100% O2 at higher than ambient pressure inside a sealed chamber 1.5 to 2 hours a day 3-5/week • Most often used for hypoxia wounds , CO poisoning , gas emboli ,scuba diving injury “ the bends” smoke inhalation • Restoration of tissue PO2 to normal/above-normal fibroblast proliferation , collagen production,angiogenesis,reduced anaerobic colonization improved phagocytosis. 25-30 SESSIONS NEEDED
- 35. Auxiliary Management • Discontinue all medications that may contribute to calciphylaxis, including vitamin D, calcium supplements, warfarin, and iron. • Kidney transplant patients may require adjustment of therapy with specific attention to avoiding agents that delay wound healing-like sirolimus/everolimus/steroid • 1 mg/kg enoxaparin twice daily demonstrated efficacy in calciphylaxis ulcer healing. • 10 mg tissue plasminogen activator (tPA) for 14 days iv. is beneficial in hypercoagulable state
- 36. Combination Treatment • Sodium thiosulfate in combination with hyperbaric oxygen therapy has shown efficacy. • Combination therapies such as sodium thiosulfate with Cinacalcet and sodium thiosulfate with bisphosphonates are currently being investigated. • Two possible molecular targets are Fetuin-A and Matrix Gla, both of which are vascular calcification inhibitorsare research approaches
- 37. Summary of treatment approaches
- 38. Complications • Complications of calciphylaxis range from moderate interference with activity to death. • Lesions of calciphylaxis frequently result in nonhealing ulcers and cutaneous gangrene. • Acral lesions may fail to heal with conservative therapy and lead to amputation. Sepsis may result from the non healing wounds. • Patients with internal involvement may develop gastrointestinal haemorrhage, infarction, or organ failure. • Patients who do not die of sepsis or organ failure frequently undergo amputation of an involved limb.
- 39. Take home message • Clinical picture is sufficient to diagnose CUA in most cases • There are high number of missed, undiagnosed cases • Optimize the dialysis prescription • Sodium thiosulfate is a first-line treatment option • Bisphosphonates is another treatment option
- 40. Take home message • Parathyroidectomy /cinacalcet are options in CUA • CUA treatment should be multimodal • Stopping vitamin K antagonist should be considered • Vitamin K supplementation may be considered • Prognosis of CUA is poor(1&5y survival rates estimated to be 45% & 35%) • Lack of evidence does not justify neglect:how can we address unmet needs in calciphylaxis?
- 41. THANK YOU