More Related Content
Similar to mohammed aiyaz
Similar to mohammed aiyaz (20)
mohammed aiyaz
- 1. Evaluation of DAA (direct-acting antiviral) access across the US:
the interplay between Hepatitis C (HCV) patients and insurance type
Jason Katz1
, Aiyaz Mohammed2
, James Deemer1
,
Elizabeth Baynton2
1
Ipsos Healthcare, New York, NY, United States,
2
Ipsos Healthcare, London, United Kingdom
Access to highly effective new Direct Acting
Antiviral (DAA) regimens containing sofosbuvir
(and/or ledipasvir) or ombitasvir/paritaprevir/
ritonavir and dasabuvir come at a high cost, making health insurance
companies reluctant to cover all patients - mitigating treatment access across
the US. This has led to several lawsuits surrounding denial of coverage of
drugs against health insurance companies who have set tight restrictions on
treatment access1
. Factors such as gender, age, severity of liver damage, and
the extent of viral load have been shown to significantly impact one’s chances
of gaining access to treatment
2
.
The aim of this study was to analyze the effect of previously associated
factors on treatment outcome using 2015 Ipsos HCV Therapy Monitor data
and Chi-squared Automatic Interaction Detection (CHAID). Here we leverage
our chart study on Hepatitis C patients and a CHAID analysis to determine
how viral load, comorbidities, substance abuse, insurance, and fibrosis score
influence treatment decisions.
1. Abram, S. (2015, June 1). Woman sues Anthem Blue Cross for denying hepatitis C drug Harvoni. Retrieved October 27, 2015.
2. Do A, Mittal Y, Liapakis A, Cohen E, Chau H, Bertuccio C, et al. (2015) Drug Authorization for Sofosbuvir/Ledipasvir (Harvoni) for Chronic HCV Infection in a Real-World
Cohort: A New Barrier in the HCV Care Cascade. PLoS ONE 10(8): e0135645. doi:10.1371/journal.pone.0135645
Ipsos Healthcare’s HCV Therapy Monitor,
running since 2005 in the USA, reports on
150 physicians per quarter across the USA.
Physicians provide patient demographic, disease and treatment data on treated
and untreated HCV patients seen within each study period. In the abstract we
used January to March 2015 data, but in this analysis we used HCV Therapy
Monitor data from January to August 2015, the months in which all sofosbuvir,
sofosbuvir+ledipasvir, and ombitasvir/paritaprevir/ritonavir and dasabuvir
regimens were available. We also added a Chi-squared Automatic Interaction
Detection (CHAID) analysis using R programming, with treatment status as
the dependent variable and fibrosis, viral load, insurance, and comorbidities
as the independent variables. All variables are categorized in order to provide
a high level view of these factors in the analysis. The CHAID analysis was
performed without a predetermined formula but was pruned to keep all
patient observations to 30 patients and above. The analysis was replicated
independently. The results section will be limited to specific branches of the
CHAID decision tree.
Premise
Methods
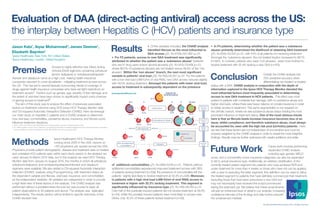
Results • Of the variables included, the CHAID analysis
identified fibrosis as the most influential to
DAA access χ2(1, N=4755)=501.462 p.01
• For F2 patients, access to new DAA treatment was significantly
attributed to whether the patient was a ‘substance abuser’ (patients
who are IV drug users and/or alcohol abusers) χ2(1, N=913)=79.856 p.01,
where 88.5% of substance abusers are not treated versus 46.4% of the ’non
abusers’. Within the ‘non abuser’ branch, the next most significant
variable is patients’ viral load χ2(2, N=782)=20.057 p.01. For the patients
with a low viral load (6M IU/ml of viral RNA), new DAA access reduces slightly
with 48.5% lacking treatment. Amongst the patients with lower viral load,
access to treatment is subsequently dependent on the presence
of additional comorbidities χ2(1, N=596)=9.518 p.01. Patients without
additional comorbidities experienced improved treatment access with 38%
of patients lacking treatment (n=158); the presence of comorbidities left the
patients slightly less likely to receive treatment at 52.3% (n=438). Moreover,
in patients with a high viral load (6M IU/ml of viral RNA) access to
treatment is higher with 32.2% lacking treatment. This segment is
significantly influenced by insurance-type χ2(1, N=146)=28.763 p.01.
Over half of the publically-insured patients did not receive treatment at 59.3%
(n=54), whilst the privately insured patients were more likely to access new
DAAs; only 16.3% of these patients lacked treatment (n=92).
Conclusion
Future Work
• In F4 patients, determining whether the patient was a substance
abuser primarily determined the likelihood of obtaining DAA treatment
χ2(1, N=834)=53.220 p.01, with 61% of all patients not receiving treatment.
Amongst the ‘substance abusers’, the not treated fraction increased to 88.1%
(n=691). In contrast, patients who were ‘non-abusers’ were more inclined to
receive treatment with 55.4% lacking a new DAA (n=143).
Overall, the CHAID analysis has
70% predictive accuracy when
differentiating non-treated vs treated
status with a DAA. CHAID analysis in conjunction with the depth of
information captured in the Ipsos HCV Therapy Monitor denoted the
most influential factors most frequently associated in determining
access to new DAA treatment in HCV patients. This effect was most
evident in patients with moderate liver damage, with no substance abuse and
higher viral loads, where there was heavy reliance on private insurance in order
to obtain access to treatment. This same segmentation is not required on
the cirrhotic branch, where we see substance abuse status holding the most
prominent influence on treatment status. One of the most obvious trends
here is that as fibrosis levels increase insurance becomes less of an
issue, whilst compliance, and therefore substance abuse, must always
be accounted for, even with the high risk pool (cirrhotic) patients. Here
we see that these factors are not independent of one another and must be
properly weighted by the CHAID analysis in order to reveal the most insightful
findings. Results may be further optimized with careful additions and edits.
Future work involves performing
expanded CHAID analysis
including age, gender, MELD
score, and a comorbidity score; insurance categories can also be expanded
to list to actual insurance type. Additionally, an arbitrary stratification of the
currently treated patient segment into patients who have achieved RVR and
under treatment for more than 4 weeks vs those who have not can be applied,
with a view to excluding the latter segment; this definition can be used to refine
the treated segment to patients that have definitely commenced their treatment,
excluding those that have been prescribed a new DAA but
may not necessarily have received the script/commenced
taking the treatment yet. We believe that these amendments
will add an enhanced level of detail to our analysis, increasing
confidence intervals of the findings and help further pinpoint
the underserved markets.
35.6%
46.4%
83.3%
68.4%
88.5%
Yes
67.5%
6M IU/ml
32.2%
52.3%
38.0%
52.5%
16.3%
88.1%
61.0%
55.4%
158
48.5%
64.1%
4755
Fibrosis Score
IPSOS HCV TM
Q1-Q3’15
pa ents
F2
F3
913
834
Is the pa ent an ‘Abuser’
Is the pa ent an ‘Abuser’
No
782
HCV viral load
596 No Yes
691
143
6M IU/ml
146
Insurance
Does the pa ent
have comorbidi es?
438
92
Private
Yes
No
F1 F4
131
40
NS
59.3%54
Government
Not Tested
1368
Sample size
% untreated
Top driver of
treatment
decision
Second er
drivers
Third er
drivers
Fourth er
drivers
All data collected online; © Ipsos 2015, all rights reserved.