
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Liver cirrhosis
Similar to Liver cirrhosis (20)
Recently uploaded
Recently uploaded (20)
Liver cirrhosis
- 1. LIVER CIRRHOSIS Pharmacy Practice To: Sir Narendar Sharma By: Mohammad Waqas Mairaj 2K16-PHA-56 (morning) Epidemiology & Etiology 2 Pathophysiology of cirrhosis 3 Clinical Presentation 5 Diagnosis 6 Treatment 7 Drug monitoring guidelines 11 Liver transplant surgery 12
- 2. 2 EPIDEMIOLOGY ❖ The Prevalence of cirrhosis in the United States was approximately 0.27%, corresponding to 633,323 adults. 69% reported that they were unaware of having liver disease. High risk groups: ➔ The prevalence was higher in non-Hispanic blacks and Mexican Americans. ➔ Diabetes, alcohol abuse, hepatitis C and B, male sex, and older age were all independently associated with cirrhosis, with a population attributable fraction of 53.5% from viral hepatitis (mostly hepatitis C), diabetes, and alcohol abuse. ❖ Mortality was 26.4% per 2-year interval in cirrhosis compared with 8.4% in propensity-matched controls. ETIOLOGY Causes of Cirrhosis maybe following: ❖ Chronic alcohol consumption. ❖ Chronic viral hepatitis (types B and C). ❖ Metabolic liver disease. ❖ Hemochromatosis, Wilson disease, antitrypsin deficiency, nonalcoholicα − 1 steatohepatitis (NASH), cystic fibrosis. ❖ Immunologic disease ❖ Autoimmune hepatitis, primary biliary cirrhosis. ❖ Vascular disease ❖ Budd-Chiari syndrome, cardiac failure. ❖ Drugs ❖ Isoniazid, methyldopa, amiodarone, dronedarone, methotrexate, tamoxifen, retinol (vitamin A), propylthiouracil and didanosine.
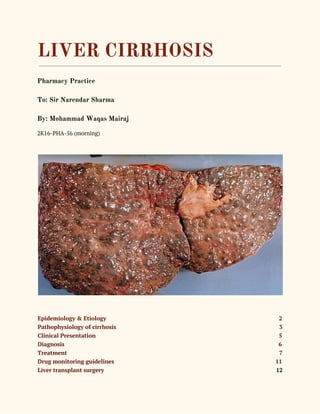
- 3. 3 PATHOPHYSIOLOGY of CIRRHOSIS ❖ Cirrhosis results in elevation of portal blood pressure because of fibrotic changes in the hepatic sinusoids, changes in the levels of vasodilator and vasoconstrictor mediators, and an increase in blood flow to the splanchnic vasculature. ❖ The pathophysiologic abnormalities that cause it results in the commonly encountered problems of ascites, portal hypertension and esophageal varices, HF and coagulation disorders. Portal hypertension and varices ❖ The most common sequelae of the portal hypertension is the development of varices and alternative routes of blood flow resulting in acute variceal bleeding. ❖ Portal hypertension is defined by the presence of a gradient of greater than 5 mm Hg between the portal and central venous pressure. ❖ Portal hypertension is characterized by the hypervolemia, Increased cardiac index, hypotension and decreased systemic vascular resistance. ❖ Progression to bleeding can be predicted by Child-Pugh score, size of the varices, and the presence of red wale markings on the varices. First variceal hemorrhage occurs at an annual rate of about 15% and carries a mortality of 7% to 15%.
- 4. 4 Hepatic Encephalopathy ❖ Hepatic encephalopathy is a metabolically induced functional disturbance of the brain that is potentially reversible. ❖ The symptoms of HE are thought to result from an accumulation of gut-derived nitrogenous substances in the systemic circulation as a consequence of shunting through portosystemic collaterals bypassing the liver. ❖ These substances then enter the central nervous system (CNS) and result in alterations of neurotransmission that affect consciousness and behavior. ❖ Type A HE is induced by acute liver failure, type B results from portal-systemic bypass without intrinsic liver disease, and type C occurs with cirrhosis. HE may be classified as episodic, persistent, or minimal.
- 5. 5 Coagulation Defects ❖ Complex coagulation derangements can occur in cirrhosis. These derangements include the reduction in the synthesis of coagulation factors, excessive fibrinolysis, disseminated intravascular coagulation, thrombocytopenia, and platelet dysfunction. ❖ Vitamin K–dependent clotting factor levels are decreased, with factor VII affected first because it has a short half-life. The net effect of these events is the development of bleeding diathesis. CLINICAL PRESENTATION Signs and Symptoms ❖ The range of presentation of patients with cirrhosis maybe from asymptomatic. ❖ Some presenting characteristics with cirrhosis are 1. Anorexia 2. Weight loss 3. Weakness 4. Fatigue 5. Jaundice 6. Pruritus 7. Gastrointestinal bleeding 8. Coagulopathy 9. Increased abdominal girth with shifting flank dullness
- 6. 6 10. Mental status changes 11. Vascular spiders 12. Gynecomastia and reduced libido 13. Ascites, edema, pleural effusion and respiratory difficulties 14. Malaise 15. Encephalopathy DIAGNOSIS Laboratory tests ❖ Hypoalbuminemia ➔ Albumin and coagulation factors are markers of hepatic synthetic activity and are used to estimate hepatocyte functioning in cirrhosis. ❖ Elevated prothrombin time (PTT) ❖ Elevated serum conjugated bilirubin indicate that the liver has lost at least half its excretory capacity. When alkaline phosphatase is elevated and aminotransferases levels are normal, elevated conjugated bilirubin is a sign of cholestatic disease. ❖ Thrombocytopenia ➔ It is found in 15% to 70% of cirrhotic patients. ❖ Elevated aspartate transaminase, alanine transaminase (ALT) ➔ These enzymes has increased concentration in plasma after hepatocellular injury ❖ Alkaline phosphatase (AST) and -glutamyl transpeptidase (GGT) are elevated in plasmaγ with obstructive disorders that disrupt the flow of bile from hepatocytes to bile ducts. Non-invasive techniques ❖ Imaging tests. Magnetic resonance elastography (MRE) may be recommended. This noninvasive advanced imaging test detects hardening or stiffening of the liver. Other imaging tests, such as MRI, CT and ultrasound, may also be done. ❖ Liver biopsy. A liver biopsy can diagnose cirrhosis when the results of other tests are uncertain. The biopsy may show the cause of cirrhosis.
- 7. 7 TREATMENT ❖ Treatment goals are clinical improvement or resolution of acute complications, such as variceal bleeding, and resolution of hemodynamic instability for an episode of acute variceal hemorrhage. ❖ Other goals are prevention of complications, adequate lowering of portal pressure with medical therapy using β-adrenergic blocker therapy, and support of abstinence from alcohol. ❖ General approach to Treatment ● Approaches to treatment include the following: ➔ Identify and eliminate the causes of cirrhosis (eg, alcohol abuse). ➔ Assess the risk for variceal bleeding and begin pharmacologic prophylaxis where ➔ indicated, reserving endoscopic therapy for high-risk patients or acute bleeding ➔ episodes. ➔ The patient should be evaluated for clinical signs of ascites and managed with ➔ pharmacologic treatment (eg, diuretics) and paracentesis. Spontaneous bacterial ➔ peritonitis (SBP) should be carefully monitored in patients with ascites who ➔ undergo acute deterioration. ➔ HE is a common complication of cirrhosis and requires clinical vigilance and ➔ treatment with dietary restriction, elimination of CNS depressants, and therapy to ➔ lower ammonia levels. ➔ Frequent monitoring for signs of hepatorenal syndrome, pulmonary insufficiency, and endocrine dysfunction is necessary. ❖ Management of PORTAL HYPERTENSION and VARICEAL BLEEDING ➔ The management of varices involves three strategies: (1) primary prophylaxis to prevent rebleeding, (2) treatment of variceal hemorrhage, and (3) secondary prophylaxis to prevent rebleeding in patients who have already bled. Primary Prophylaxis ➔ All patients with cirrhosis and portal hypertension should be screened for varices on diagnosis. ➔ The mainstay of primary prophylaxis is the use of a nonselective β-adrenergic blocking agent such as propranolol or nadolol. These agents reduce portal pressure by reducing portal venous inflow via two mechanisms: decrease in cardiac output and decrease in splanchnic blood flow.
- 8. 8 ➔ Therapy should be initiated with propranolol, 20 mg twice daily, or nadolol, 20 to 40 mg once daily, and titrated every 2 to 3 days to maximal tolerated dose to heart rate of 55 to 60 beats/min. ➔ Patients with contraindications to therapy with nonselective β-adrenergic blockers (i.e, those with asthma, insulin-dependent diabetes with episodes of hypoglycemia, and peripheral vascular disease) or intolerance to β-adrenergic blockers should be considered for alternative prophylactic therapy with EVL. [Endoscopic variceal ligation (EVL) is widely used to prevent esophageal variceal bleeding in patients with advanced cirrhosis]. Management of ACUTE VARICEAL HEMORRHAGE ❖ Initial treatment goals include (1) Adequate blood volume resuscitation, prompt stabilization of blood volume to maintain hemoglobin of 8 g/dL with volume expansion to maintain systolic blood pressure of 90 to 100 mm Hg and heart rate of less than 100 beats/min is recommended. ➔ Fluid resuscitation involves colloids initially and subsequent blood products. Vigorous resuscitation with saline solution should generally be avoided. (2) protection of the airway from aspiration of blood, Airway management is critical. (3) correction of significant coagulopathy and / or thrombocytopenia with fresh frozen plasma and platelets, (4) prophylaxis against SBP and other infections, (5) control of bleeding, (4) prevention of rebleeding, (5) preservation of liver function. ❖ Combination pharmacologic therapy plus EVL or sclerotherapy (when EVL is not technically feasible) is the most rational approach to treatment of acute variceal bleeding. ❖ Octreotide is administered as an IV bolus of 50 mcg followed by a continuous infusion of 50 mcg/h. It should be continued for 5 days after acute variceal bleeding. (Patients should be monitored for hypo- or hyperglycemia). ❖ Vasopressin, alone or in combination with nitroglycerin, is not recommended as a first line therapy for the management of variceal hemorrhage. ❖ Antibiotic therapy should be used early to prevent sepsis in patients with signs of infection or ascites. A short course (up to 7 days) of oral norfloxacin 400 mg twice daily or IV ciprofloxacin is recommended.
- 9. 9 ❖ If standard therapy fails to control bleeding, a salvage procedure such as balloon tamponade (with a Sengstaken-Blakemore tube) or transjugular intrahepatic portosystemic shunt (TIPS) is necessary. Prevention of BLEEDING A nonselective β-adrenergic blocker along with EVL is the best treatment option for prevention of rebleeding. ❖ Propranolol may be given at 20 mg twice daily (or nadolol, 20–40 mg once daily) and titrated weekly to achieve a goal of heart rate 55 to 60 beats/min. Ascites ❖ The therapeutic goals for patients with ascites are to control the ascites, prevent or relieve ascites-related symptoms (dyspnea and abdominal pain and distention). ❖ If the serum–ascites albumin gradient is greater than 1.1 g/dL (>11 g/L), the patient almost certainly has portal hypertension. ➔ The treatment of ascites secondary to portal hypertension includes abstinence from alcohol, sodium restriction (to 2 g/day), and diuretics. A goal of therapy is to increase urinary excretion of sodium to greater than 78 mmol/day. ❖ Diuretic therapy should be initiated with single morning doses of spironolactone, 100 mg, and furosemide, 40 mg, titrated every 3 to 5 days, with a goal of 0.5 kg maximum daily weight loss. The dose of each can be increased together, maintaining the 100:40 mg ratio, to a maximum daily dose of 400 mg spironolactone and 160 mg furosemide. ❖ Liver transplant should be considered in patients with refractory ascites.
- 10. 10 Spontaneous bacterial peritonitis ❖ Antibiotic therapy for the prevention of spontaneous bacterial peritonitis (SBP) should be considered in all patients who experience variceal hemorrhage and those with low-protein ascites. ❖ Patients with documented or suspected SBP should receive broad-spectrum antibiotic therapy to cover Escherichia coli, Klebsiella pneumoniae, and Streptococcus pneumoniae. ❖ Cefotaxime 2 g every 8 hours, or a similar third-generation cephalosporin for 5 days is considered the drug of choice. Oral ofloxacin, 400 mg every 12 hours for 8 days, is equivalent to IV cefotaxime. Hepatic Encephalopathy Treatment Goals: Episodic and Persistent Hepatic Encephalopathy Episodic HE Persistent HE Control precipitating factor Reverse encephalopathy Reverse encephalopathy Avoid recurrence Hospital/inpatient therapy Home/outpatient therapy Maintain fluid and hemodynamic support Manage persistent neuropsychiatric abnormalities Manage chronic liver disease Expect normal mentation after recovery High prevalence of abnormal mentation after recovery. ❖ To reduce blood ammonia concentrations in episodic HE, lactulose is initiated at 45 mL orally every hour (or 300 mL lactulose syrup with 700 mL water given as a retention enema held for 60 minutes) until catharsis begins. The dose is then decreased to 15 to 30 mL orally every 8 to 12 hours and titrated to produce two or three soft stools per day. ❖ Antibiotic therapy with metronidazole or neomycin is reserved for patients who have not responded to diet and lactulose. Rifaximin 550 mg twice daily plus lactulose can be used for patients with inadequate response to lactulose alone. ❖ Zinc acetate supplementation (220 mg twice daily) is recommended for long-term management in patients with cirrhosis who are zinc deficient.
- 11. 11 DRUG MONITORING GUIDELINES Drug Adverse Drug Reaction Monitoring Parameter Comments Nonselective β-adrenergic blocker Heart failure, bronchospasm, glucose intolerance BP, HR Goal HR: 55–60 beats/ min or maximal tolerated dose Nadolol or propranolol Octreotide Bradycardia, hypertension, arrhythmia, abdominal pain BP, HR, EKG, abdominal pain Vasopressin Myocardial ischemia/ infarction, arrhythmia, mesenteric ischemia, ischemia of the limbs, cerebrovascular accident EKG, distal pulses, symptoms of myocardial, mesenteric, or cerebrovascular ischemia/infarction Spironolactone/ furosemide Electrolyte disturbances, dehydration, renal insufficiency, hypotension Serum electrolytes (especially potassium), SCr, blood urea nitrogen, BP Goal sodium excretion: >78 mmol/day Spot urine sodium concentration greater than potassium concentration correlates well with daily sodium excretion >78 mmol/day Lactulose Electrolyte disturbances Serum electrolytes Goal number of soft stools per day: 2–3 Neomycin Ototoxicity, nephrotoxicity SCr, annual auditory monitoring Metronidazole Neurotoxicity Sensory and motor neuropathy
- 12. 12 LIVER TRANSPLANT SURGERY ❖ In advanced cases of cirrhosis, when the liver ceases to function, a liver transplant may be the only treatment option. ❖ A liver transplant is a procedure to replace your liver with a healthy liver from a deceased donor or with part of a liver from a living donor. ❖ Candidates for a liver transplant have extensive testing to determine whether they are healthy enough to have a good outcome following surgery. ❖ Historically, those with alcoholic cirrhosis have not been liver transplant candidates because of the risk that they will return to harmful drinking after transplant. ❖ For transplant to be an option if you have alcoholic cirrhosis, you would need: ➔ To find a program that works with people who have alcoholic cirrhosis ➔ To meet the requirements of the program, which would include lifelong commitment to alcohol abstinence as well as other requirements of the specific transplant center. REFERENCES ➢ Pharmacotherapy handbook 9th edition ➢ Cirrhosis - Diagnosis and treatment - Mayo clinic ➢ Pubmed.gov (The Epidemiology of Cirrhosis in the United States: A Population-based Study)