1. The Effect of Statins on Functional Mobility and Flexibility
in Healthy Masters Swimmers
Kevin Cook1, Mary Vang2, and Lisa Ferguson-Stegall, PhD1
1Hamline University, Dept. of Biology, Integrative Physiology Lab, Saint Paul, MN
2Century College, White Bear Lake, MN
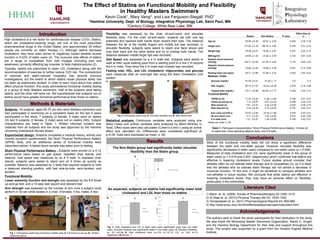
The Non-Statin group had significantly better shoulder
flexibility than the Statin group.
Flexibility was assessed by the chair sit-and-reach and shoulder
flexibility tests. For the chair sit-and-reach, subjects sat with one leg
extended and reached both hands down toward their toes. The distance
between the tip of the middle fingers and middle toe was recorded. In
shoulder flexibility, subjects were asked to reach one hand above and
over their back and the other below and try to overlap both hands. The
distance between middle finger tips was recorded.
Gait Speed was assessed by a 4 m walk test. Subjects were asked to
walk at their usual walking pace from a starting point to a line 2 m beyond
the 4 m mark. Time when the 4 m mark was crossed was recorded.
Fasting total, HDL, and LDL cholesterol, triglycerides, and glucose
were measured after an overnight fast using the Alere Cholestech LDX
system.
Methods & Materials
Conclusions
Literature Cited
Introduction
Results
Subjects: 16 subjects, aged 55-75 yrs who were Masters swimmers and
had participated in swimming on a consistent basis for the last 5 years
participated in the study. 7 subjects (2 female, 5 male) were on statins
(S) and 9 subjects (3 female, 6 male) were not on statins (NS). Subject
characteristics are listed in Table. 1. Written informed consent was
obtained from all subjects and the study was approved by the Hamline
University Institutional Review Board.
Experimental design: Subjects completed a medical history, activity and
muscle symptom questionnaire, the Short Physical Performance Battery
(SPPB) tests, and an additional series of functional mobility tests
(described below). A fasted blood sample was taken prior to testing.
Short Physical Performance Battery : Subjects were scored on a 0-12
performance value based on gait speed, repeated chair stands, and
balance. Gait speed was measured by an 8 ft walk. In repeated chair
stands, subjects were asked to stand and sit 5 times as quickly as
possible. Balance was assessed by 3 tests that required subjects to hold
a balanced standing position, with feet side-by-side, semi-tandem, and
tandem.
Functional Mobility:
Lower extremity function and strength was assessed by the 8-ft timed
up-and-go test, and a 10-step stair ascent and descent test.
Arm strength was assessed by the number of arm curls a subject could
perform in 30 sec while seated in a chair. (Females, 5 lbs; males, 8 lbs)
Acknowledgements
Statins Non Statins P value
Effect Size (d,
r)
Age (y) 64.86 ±2.38 62.67 ± 2.02 0.246 0.35, 0.18
Height (cm) 177.62 ±3.19 180.76 ± 3.82 0.276 0.31, 0.16
Weight (kg) 79.59 ±6.51 76.28 ± 3.91 0.327 0.22, 0.12
BMI (kg/m2) 24.95 ±1.29 23.29 ± 0.79 0.134 0.57, 0.29
Systolic blood pressure
(mmHg) 128.71 ±5.55 121.56 ± 2.82 0.119 0.60, 0.30
Diastolic blood pressure
(mmHg) 75.86 ±2.54 74.89 ± 2.30 0.391 0.14, 0.08
Resting heart rate (bpm) 55.71 ±2.68 51.89 ± 3.32 0.203 0.44, 0.23
Metabolic Profile
Glucose (mg/dL) 91.00 ±3.31 91.00 ± 17 0.5 0, 0
HDL (mg/dL) 60.14 ±7.57 63.22 ±6.38 0.379 0.16, 0.08
Triglycerides (mg/dL) 75.71 ±6.98 82.00 ±11.77 0.338 0.22, 0.12
Functional Mobility
*SPPB (0-12) 11.57 ±0.20 11.56 ±.029 0.758 0.01, 0.01
Timed up-and-go (s) 7.31 ±0.67 6.81 ±0.42 0.258 0.33, 0.16
Stair ascent (s) 3.91 ±0.37 4.25 ±0.26 0.222 0.38, 0.19
Stair descent (s) 3.43 ±0.29 3.73 ±0.20 0.197 0.44, 0.21
Arm curls (curl/30 s) 23.57 ±2.83 23.39 ±1.98 0.479 0.03, 0.01
Sit and reach (cm) 3.71 ±3.33 7.44 ±3.05 0.212 0.42, 0.20
4 m walk (m/s) 1.21 ±0.07 1.29 ±0.06 0.194 0.43, 0.21
Values are mean ± SE.
Statistical analysis: Continuous variables were analyzed using one
tailed t-tests and ordinal variables were analyzed by Mann-Whitney U
Tests. Effect sizes were also calculated (Cohen’s d and r) using an online
effect size calculator (4). Differences were considered significant at
p<0.05. Data were expressed as mean ± SE.
As expected, subjects on statins had significantly lower total
cholesterol and LDL than those on statins.
Table 1. Participant characteristics.*Short Physical Performance Battery; 5 times sit-
to-stand test, three standing balance tests, and 8 ft walk.
0.00
50.00
100.00
150.00
200.00
250.00
TotalCholesterol(mg/dL)
Statins
Non-Statins
0.00
20.00
40.00
60.00
80.00
100.00
120.00
140.00
LDL(mg/dL)
Statins
Non-Statins
A
B C
Fig. 3. Total cholesterol and LDL in statin users were significantly lower than non statin
users. Shoulder flexibility was significantly better in non statin users. A: Shoulder Flexibility;
p= .03, d=0.96 B: Total cholesterol level; p=.019, d=1.22 C: LDL; p= .003, d=1.6
Significant differences: §.
§
§
Fig. 2 Participants performing A: Shoulder flexibility and B: Stair ascent test.
Fig 1. Participants performing functional mobility tests A: 8-ft timed-up-and-go B: Tandem
balancing stance.
A B
BA
High cholesterol is a risk factor for cardiovascular disease (CVD). Statins,
which are cholesterol-lowering drugs, are one of the most prescribed
pharmaceutical drugs in the United States, and approximately 25 million
people are currently on statin therapy (1). Although statins decrease
cholesterol, they have been shown to negatively impact skeletal muscle
function in 5-22% of statin users (2). The muscular side effects of statins
are a range of myopathies from mild myalgia (including pain and
weakness), primarily affecting leg muscles, to fatal rhabdomyolysis (2).
Typically, statins are prescribed to lower LDL cholesterol along with the
recommendation of exercise to further reduce CVD risk. The contradiction
of exercise and statin-induced myopathy has spurred previous
investigations, but the extent to which statins impair physical ability has
not been as extensively studied. In order to learn more about how statins
affect physical function, this study administered functional mobility testing
to a group of older Masters swimmers. Half of the subjects were taking
statins, and the other half were not. We hypothesized that subjects not on
statins would have greater functional performance than those on statins.
The authors wish to thank the study participants for their dedication to the study.
We also thank the Minnesota Master Swimmers Organization, Martin C. Knight,
and the Hamline Biology Department for their help and support throughout this
study. This project was supported by a grant from the Howard Hughes Medical
Institute.
Most of the functional mobility tests did not show a significant difference
between the statin and non-statin groups. However, shoulder flexibility was
significantly decreased in statin users compared to non-statin users (p = 0.036).
Measures of total cholesterol and LDL were significantly lower in the group of
statin users (p = 0.019 and 0.003, respectively) which confirmed that statins are
effective in lowering cholesterol levels. Future studies should consider that
athletes often do not tolerate statin therapy due to myopathies (3), so it is likely
that the athletes who do tolerate statin therapy will not exhibit a decrease in
muscular function. To this end, it might be beneficial to compare athletes and
non-athletes in future studies. We conclude that while statins are effective in
lowering cholesterol levels, they may have an adverse effect on flexibility,
particularly in the extremities.
-21.00
-16.00
-11.00
-6.00
-1.00
ShoulderFlexibility(cm)
Statins Non-Statins
§
1) Mann et. Al. (2008) Annals of Pharmacotheraphy 42:1208–1215.
2) Di Stasi et. al. (2010) Physical Therapy 90(10): 1530–1542.
3) Tomaszewski et. al. (2011) Pharmacological Reports 63: 859-866.
4) http://www.polyu.edu.hk/mm/effectsizefaqs/calculator/calculator.html
Editor's Notes
T test on the SF12 totall = .054
Exahustion was analyzed via Wilcoxon