Brachial Plexus Injury Diagnosis and Treatment
•Download as PPTX, PDF•
1 like•60 views

brachial plexus injury

Recommended
More Related Content
Similar to Brachial Plexus Injury Diagnosis and Treatment
Similar to Brachial Plexus Injury Diagnosis and Treatment (20)
Recently uploaded
Recently uploaded (20)
Brachial Plexus Injury Diagnosis and Treatment
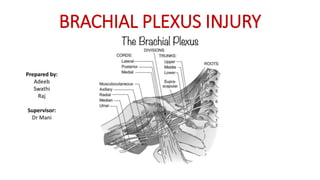
- 1. BRACHIAL PLEXUS INJURY Prepared by: Adeeb Swathi Raj Supervisor: Dr Mani
- 2. Brachial plexus Nerve plexus formed by confluence of nerve roots from C5-T1.
- 6. DEFINITION ● Sudden damage to brachial plexus causing weakness, loss of feeling or movement in the shoulder, arm or hand ● Injuries to the brachial plexus can occur in one or more of these areas ● Spinal Nerves ● Trunks ● Divisions ● Cords ● Branches
- 7. It is important to establish 1. Level of lesion 2. Type of damage 3. Pre vs post ganglionic
- 8. NERVE INJURY CLASSIFICATION Low energy injury – neuropraxia High energy injury / open wound – axonotmesis/neurometsis
- 10. CLASSIFICATION • PREGANGLIONIC -avulsion proximal to dorsal root ganglion • POSTGANGLIONIC -occurs distal to dorsal root ganglion
- 11. Pre-ganglionic Lesions • Disruption of nerve roots proximal to the dorsal root ganglion • Cannot recover or surgically irreparable • Features: Burning pain in an anesthetic hand Paralysis of scapular muscles elevated hemidiaphragm (phrenic nerve) denervation of cervical paraspinal muscles seen in electromyography examinations Horner’s syndrome Absence of Tinel’s sign Severe vascular injury Associated fracture of the cervical spine Spinal cord dysfunction
- 12. Pre-ganglionic Lesions • Histamine test: POSITIVE Afferrent axons remain intact Normal triple response with flare seen (redness, wheal, flare) • CT myelography or MRI: pseudomeningoceles produced by root avulsion
- 13. Pre-ganglionic Lesions Horner’s syndrome – disruption of symptathetic chain (C8/T1 avulsion) Drooping of eyelid Pupillary constriction Anhidrosis
- 14. loss of serratus anterior (long thoracic nerve) leads to medial winging loss of rhomboids (dorsal scapular nerve) leads to lateral winging
- 15. Post-ganglionic Lesions • Can be repaired and capable of recovery • Histamine test: NEGATIVE (continuity between skin & dorsal root ganglion interrupted)
- 17. AETIOLOGY OF BRACHIAL PLEXUS INJURY
- 18. • TRAUMATIC PLEXOPATHIES - High speed collision - Direct blow to the shoulder region - Gunshot - Laceration/ animal bite • NON- TRAUMATIC PLEXOPATHIES - Neoplastic and radiation-induced brachial plexopathy - Thoracic outlet syndrome • OBSTETRIC INJURY - Erb’s palsy - Klumpke’s palsy
- 20. BURNER SYNDROME • Is a transient neurapraxia resulting from a stretch or compression of the upper roots of the brachial plexus. • Three mechanisms of burners are known: ●The first is traction injury to the brachial plexus, which occurs when the shoulder is depressed and the neck is forced laterally away from the involved side, stretching the brachial plexus ●The second is a direct blow to the supraclavicular fossa ●The third is nerve compression by a combination of neck hyperextension and ipsilateral lateral flexion
- 22. NEOPLASTIC AND RADIATION-INDUCED BRACHIAL PLEXOPATHY • Neoplastic plexopathies can result from direct pressure by a local cancer mass • Pain in the shoulder and axilla is the most common presenting symptom of neoplastic brachial plexopathy. • Invasion of the lower plexus (inferior trunk and medial cord) occurs more frequently than invasion of the upper trunk. • The toxic effects of radiation may injure axons directly causing ischemic changes to axons with multifocal denervation.
- 30. INVESTIGATION • Plain radiograph • CT Myelography/MRI • Electrodiagnostic test • Electromyography (EMG) • Nerve conduction velocity studies (NCV)
- 31. * Plain radiograph • Chest (inspiratory) • Clavicle • Cervical spine • Scapular and shoulder series
- 32. CT Myelography • Gold standard to identify root avulsions • Important findings • Pseudomeningocele • Absence of roots • Should be done 3-4 weeks post trauma • To ensure there is enough time for blood clots to be absorbed CT myelogram shows absence of the affected nerve roots (arrow) and the intact nerve roots on the unaffected side (arrowheads).
- 34. * MRI Neurotmesis. A 43-year-old woman with loss of function in the left upper extremity following recent neck surgery - shows severed, enlarged, and hyperintense C5 and C6 nerve roots with distal end bulb neuromas (arrows), just proximal to the formation of the left upper trunk.
- 35. Electrophysiology Studies (EPS) • Electromyography (EMG) • More sensitive towards motor nerves • Nerve conduction studies (NCS) • More sensitive towards sensory nerves • Sensory nerve action potentials (SNAPs) helps to localize lesions • Preserved in pre-ganglionic lesions • Absent in post-ganglionic or combined pre and post-ganglionic lesions • Serial EPS helps to assess progress of recovery / re-innervation
- 39. Conservative Management • Aim • Maintain range of motion of extremities • Strengthen the remaining functional muscles • Protect denervated dermatomes • Manage Pain Immobilise : Splint and sling (decrease the edema) Physiotherapy : Joint mobility, muscle strength Pain Management
- 40. Splint / Orthosis • Aim • Prevent subluxation of shoulder joint • Prevent contractures • Cosmesis • Types • Flail Arm Splint • Wilmer Orthosis • Stanmore Orthosis • Dynamic Assist Elbow Flexion Orthosis
- 41. Surgical Management Aim of surgery : 1. Restore elbow flexion 2. Restore shoulder abduction, stability of shoulder 3. Elbow extension 4. Restore wrist extension 5. Restore finger flexion
- 42. Timing of surgical intervention Immediate (<1week) Late (3 - 6months) ● Vascular injury ● Open penetrating injury ● Open infected crushing/stretching wounds ● Complete traumatic palsy of C5-T1 roots • Traumatic palsy injuries with no clinical sign of functional restoration or electromyography signs of denervation. • Plateau in neurologic recovery
- 43. Modes of surgical intervention Direct End to End Repair Nerve grafting Nerve transfer
- 44. Direct End to End Repair • Usually only possible for acute and sharp penetration injuries • Types • Group fascicular repair • Epineural repair • Perineural repair
- 45. Nerve grafting •Transfer of donor nerve from other part of the body to replace the damaged nerve •Donor sites: 1.Sural nerve 2.Sensory branch of ulnar nerve 3.Medial cutaneous nerve of forearm •Predominantly used in clear cut injuries with healthy proximal stump and with no axial damage
- 47. Neurotization (Nerve Transfer) • For preganglionic root injury • A healthy but less valuable nerve is transferred in order to reinnervate a more important motor territory that has lost its innervation through irreparable damage to its nerve • Motor branches are used as donor
- 50. * Intraoperative picture showing musculocutaneous nerve neurotization by three intercostal nerves
- 51. *
- 52. * Secondary Operation Tendon Transfer Muscle Transfer Arthrodesis • need in the absence of spontaneous recovery or when the first surgical procedure does not provide satisfactory outcomes
- 53. * Free functioning muscle transplantation • Transplant of a muscle with its neurovascular pedicle to a new location • Gracilis muscle - to restore elbow flexion • Alternative muscle • Rectus femoris • Lats dorsi
- 54. *
- 55. * Tendon Transfer • Upper or lower brachial plexus traumatic injury with only partial paralysis • Goal is to restore good muscle strength through a ROM of 30- 130’
- 56. * Arthrodesis • Done as the last resort • Usually reserved for unstable or painful shoulder • To achieve shoulder stability
- 57. Targeted Muscle Reinnervation • To provide intuitive prosthetic control to upper extremity amputees • Rely on signals acquired from muscles just above the amputation sites
- 59. Post-op Care Surgical Exploration and Primary Intervention Rehab and Reassess. Migrating Tinel sign? If No, Re- explore +/- Nerve Reconstruction Rehab and Reassess If No Improvement, Secondary Intervention Rehab and Reassess Joint Fusion / Splinting
- 60. * Prognosis • Regeneration of nerve ~1mm/day • Recovery of BPI may take up to 3 years • Better prognosis – Upper plexus injury (hand preserved function) • Poor prognosis – root avulsion (pre-ganglionic), not repairable
- 61. References • Apley’s Orthopedics • Hsueh, Y.-H., & Tu, Y.-K. (2020). Surgical Reconstructions for adult brachial plexus injuries. Part I: Treatments for combined C5 and C6 injuries, with or without C7 injuries. Injury. • Maldonado, A. A., Kircher, M. F., Spinner, R. J., Bishop, A. T., & Shin, A. Y. (2017). Free Functioning Gracilis Muscle Transfer With and Without Simultaneous Intercostal Nerve Transfer to Musculocutaneous Nerve for Restoration of Elbow Flexion After Traumatic Adult Brachial Pan- Plexus Injury. The Journal of Hand Surgery, 42(4), 293.e1–293.e7. • Seal, A., & Stevanovic, M. (2011). Free Functional Muscle Transfer for the Upper Extremity. Clinics in Plastic Surgery, 38(4), 561–575.
- 62. • Sakellariou, Vasileios I et al. “Treatment options for brachial plexus injuries.” ISRN orthopedics vol. 2014 314137. 14 Apr. 2014 • Wolford, Larry M, and Eber L L Stevao. “Considerations in nerve repair.” Proceedings (Baylor University. Medical Center) vol. 16,2 (2003): 152-6