Got Pain AMIA Poster 2013
•
0 likes•168 views

A study of veterans with chronic noncancer pain found associations between increased opioid dosage and higher rates of adverse effects. Interviews with providers showed inconsistent practices in assessing opioid risk, obtaining written agreements, and conducting functional assessments. To improve outcomes, the presentation recommends clinical decision support with structured data entry at the point of care, periodic assessments, education on guidelines, and multidisciplinary treatment approaches that favor non-opioid therapies over chronic opioid use whenever possible.
Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Got Pain AMIA Poster 2013
Similar to Got Pain AMIA Poster 2013 (20)
Got Pain AMIA Poster 2013
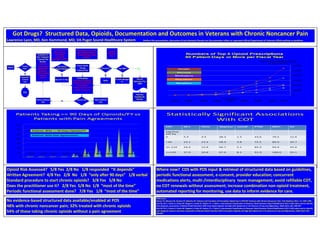
- 1. Got Drugs? Structured Data, Opioids, Documentation and Outcomes in Veterans with Chronic Noncancer Pain Lawrence Lyon, MD, Ken Hammond, MD, VA Puget Sound Healthcare System Neither this presentation, discussion of any elements therein nor the presenter reflect or represent official Department of Veterans Affairs policies or positions • . Statistically Significant Associations With COT COT AE’s Clinic ‘depress’ ‘suicid’ PTSD MD’s SU Mg/Day MS Eq 0 5.4 4.5 38.3 1.3 43.6 70.5 12.6 <40 13.1 13.4 58.9 3.8 72.5 89.0 20.7 41-119 24.4 12.8 66.7 5.1 83.3 94.9 25.6 >=120 27.0 10.8 67.6 8.1 91.9 100.0 35.1 Opioid Risk Assessed? 5/8 Yes 2/8 No 1/8 responded “It depends” Written Agreement? 4/8 Yes 2/8 No 1/8 “only after 90 days” 1/8 verbal Standard procedure to start chronic opioids? 3/8 Yes 5/8 No Does the practitioner use it? 2/8 Yes 5/8 No 1/8 “most of the time” Periodic functional assessment done? 7/8 Yes 1/8 “most of the time” Chronic Pain? Evaluation of Acute Pain Stop Evaluation of Prior Treatment/ Treatment Plan Revision Opioid Risk Assessment; Mental Health Diagnoses; Patients receive additional treatment? Use Chronic Opioid Therapy? Non-COT Tx Plan Chronic Opioid Therapy Treatment Plan F/U Evaluation Functional Assessment; Primary Care Visits/Year; F/U Frequency Adverse Outcomes, Side Effects, Pain Burden Outcome OK? Schedule II? Refills Pharmacy Facilitates Rx RenewalRevise Treatment Plan Keep Treatment Plan Narcotic Medication Plan (NMP) No No Yes Yes No Use NMP? YesYes Provider Manages Rx No Time to Chronic Opioid Therapy, Clinic Usage, concurrent medications, eg BZ’s Opioid High vs Low Dose, eg >120mg MS Eq/day vs <40mg MS Eq/day, Refills/ Renewals Narcotic Medication Plan? Patient Yes No References: Macey TA, Morasco BJ, Duckart JP, Dobscha SK. Patterns and Correlates of Prescription Opioid Use in OEF/OIF Veterans with Chronic Noncancer Pain. Pain Medicine 2011; 12; 1502-1509. Seal KS, Shi Y, Cohen G, Cohen BE, Maguen S, Krebs EE, Neylan TC. e-Table 1, International Classification of Diseases, Ninth Revision Clinical Modification (ICD-9-CM) codes used to identify pain diagnosis, Association of Mental Health Disorders With Prescription Opioids and High-Risk Opioid Use in US Veterans of Iraq and Afghanistan, JAMA 2012; 307; 940-947. Seal KS, Shi Y, Cohen G, Cohen BE, Maguen S, Krebs EE, Neylan TC. e-Table 2, International Classification of Diseases, Ninth Revision Clinical Modification (ICD-9-CM) codes used to identify and categorize adverse outcomes, Association of Mental Health Disorders With Prescription Opioids and High-Risk Opioid Use in US Veterans of Iraq and Afghanistan, JAMA 2012; 307; 940-947. No evidence-based structured data available/enabled at POS 48% with chronic noncancer pain; 32% treated with chronic opioids 54% of those taking chronic opioids without a pain agreement Where now? CDS with POS input & retrieval of structured data based on guidelines, periodic functional assessment, e-consent, provider education; concurrent medications alerts, multi-/interdisciplinary team management; avoid refillable COT, no COT renewals without assessment; increase combination non-opioid treatment, automated reporting for monitoring, use data to inform evidence for care.