Recommended

Recommended
More Related Content
What's hot
What's hot (16)
Similar to NYSACCP_Kristin_Yin_Nov2016
Similar to NYSACCP_Kristin_Yin_Nov2016 (20)
NYSACCP_Kristin_Yin_Nov2016
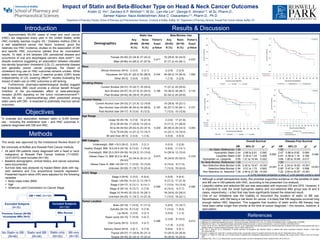
- 1. Introduction Objectives Results & Discussion • Although a small retrospective study, this provides supportive evidence on the benefits of statin and BB use in DM patients with HNC, according to the presented Cox analysis. • Lipophilic statins and selective BB use was associated with improved OS and DFS. However, it is important to note the small hydrophilic statins and non-selective BBs group size (6 and 8 cases, respectively) – a fact that may have significantly biased the observed result. • One of our limitations was the inability to document the duration of statin or BB use. Nevertheless, with DM being a risk factor for cancer, it is likely that DM diagnosis occurred long enough before HNC diagnosis. This suggests that duration of statin and/or BB therapy may have been rather longer than shorter at the time of cancer diagnosis – this remains, however, a speculation. Impact of Statin and Beta-Blocker Type on Head & Neck Cancer Outcomes Kristin Q. Yin1, Zachary A.P. Wintrob1,2, M.Sc., Lan-Hsi Lin1, George K. Nimako1,2, M.Sc, Pharm.D., Sameer Kapoor, Naza Abdelrahman, Alice C. Ceacareanu1,2, Pharm.D., Ph.D. 1Department of Pharmacy Practice, School of Pharmacy and Pharmaceutical Sciences, University at Buffalo, Buffalo, NY, 2Department of Pharmacy Services, Roswell Park Cancer Institute, Buffalo, NY Methods Approximately 60,000 cases of head and neck cancer (HNC) are diagnosed every year in the United States, while HNC mortality reaches roughly 4%.1 Diabetes mellitus (DM) is a well established cancer risk factor; however, given the relatively low HNC incidence, studies on the association of DM and specific HNC occurrence yielded thus far inconsistent results. To date, a link between DM, periodontal disease and occurrence of oral and esophageal cancers does exist2-4, but despite evidence suggesting an association between elevated low-density lipoprotein cholesterol (LDL-C), periodontal disease and generally poorer cancer prognosis, the impact of cholesterol drug use on HNC outcomes remains unclear. While statins were reported to lower C-reactive protein (CRP) levels independently of LDL lowering effect5,6, studies evaluating the impact of statin use on HNC outcomes is still lacking. Furthermore, pharmaco-epidemiological studies suggest that β-blockers (BB) could provide a clinical benefit through inhibition of the pro-metastatic effect of beta-adrenergic receptor (β-AR) signaling on the tumor microenvironment7,8. Hence, BB use – pharmacotherapy often prescribed among statin users with DM - is expected to potentially improve cancer outcomes. To evaluate any association between statin or β-AR blocker use - including the medication type – and HNC outcomes in patients diagnosed with DM and HNC. This study was approved by the Institutional Review Board of the University at Buffalo and Roswell Park Cancer Institute. • All adult DM patients newly diagnosed with a head or neck malignancy at Roswell Park Cancer Institute (1/1/2003- 12/31/2010) were included (N=130) • Baseline demographic, clinical history, and cancer outcomes were documented. • Survival data was analyzed by Kaplan-Meier plots with log- rank statistics and Cox proportional hazards regression. Presented hazard ratios (HR) were adjusted for the following variables Body mass index (BMI) Age American Joint Commission on Cancer Stage References 1. Figueiredo RA, Weiderpass E, Tajara EH, et al. Diabetes mellitus, metformin and head and neck cancer. Oral Oncol. 2016;61:47-54. 2. Migliorati CA. Periodontal diseases and cancer. The Lancet Oncology. 2008;9(6):510-2. doi: 10.1016/S1470-2045(08)70138-4. PubMed PMID: 18510985. 3. Fitzpatrick SG, Katz J. The association between periodontal disease and cancer: a review of the literature. Journal of dentistry. 2010;38(2):83-95. 4. Yang X, So W, Ko GTC, Ma RCW, Kong APS, Chow CC, et al. Independent associations between low-density lipoprotein cholesterol and cancer among patients with type 2 diabetes mellitus. Canadian Medical Association Journal. 2008;179(5):427-37 5. MC, Ahn Y, Jang SY, et al. Comparison of clinical outcomes of hydrophilic and lipophilic statins in patients with acute myocardial infarction. Korean J Intern Med. 2011;26(3):294-303. 6. Kruse AL, Luebbers HT, Gratz KW. C-reactive protein levels: a prognostic marker for patients with head and neck cancer? Head Neck Oncol. 2010;2:21. 7. Watkins JL, Thaker PH, Nick AM, et al. Clinical impact of selective and nonselective beta-blockers on survival in patients with ovarian cancer. Cancer. 2015;121(19):3444- 3451. 8. Eskander R BL, Chiu C, et al. Beta blocker use and ovarian cancer survival: a retrospective cohort. Gynecol Oncol. 2012;127(1):21. DM + HNC (N=160) Included Subjects (N=130) MRs Review BB only (N=18) Excluded Subjects (N=30) Previous Cancer (N=28) Incomplete MRs (N=2) Statin only (N=32) Statin and BB (N=34) No Statin or BB (N=46) Overall Survival Disease-Free Survival HR 95% CI p1 p2 HR 95% CI p1 p2 No Statin (Reference) 1.00 - - 0.062 1.00 - - 0.048 Hydrophilic Statin 2.44 0.86 to 6.91 0.092 2.47 0.88 to 6.92 0.084 Lipophilic Statin 0.69 0.39 to 1.23 0.208 0.67 0.38 to 1.18 0.168 Hydrophilic vs. Lipophilic 3.55 1.21 to 10.44 0.022 3.68 1.26 to 10.69 0.017 No Beta-Blocker (Reference) 1.00 - - <0.001 1.00 - - <0.001 Non-Selective Beta-Blocker 6.86 2.42 to 19.47 <0.001 6.14 2.24 to 16.83 <0.001 Selective Beta-Blocker 0.94 0.51 to 1.72 0.845 0.85 0.47 to 1.55 0.598 Non-Selective vs. Selective 7.28 2.46 to 21.58 <0.001 7.22 2.50 to 20.87 <0.001 p1 is the individual comparison p-value, p2 is the adjusted overall p-value.