
Recommended
More Related Content
Similar to Case_Studies_in_Emergency_Medicine_Trauma_-_Lisa_Yosten,_MD.pdf
Similar to Case_Studies_in_Emergency_Medicine_Trauma_-_Lisa_Yosten,_MD.pdf (20)
Recently uploaded
Recently uploaded (20)
Case_Studies_in_Emergency_Medicine_Trauma_-_Lisa_Yosten,_MD.pdf
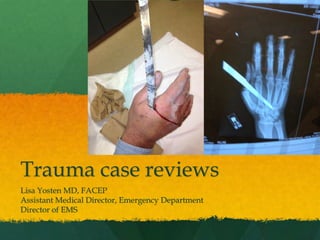
- 1. Trauma case reviews Lisa Yosten MD, FACEP Assistant Medical Director, Emergency Department Director of EMS
- 2. Case #1 EMS bringing “stab wound” to abdomen, 2 am “10 inch knife” Full trauma alert activated 25 y/o hispanic male stabbed left lower flank and left upper quadrant, intoxicated GCS 14, verbalizing, not cooperative. VS: 90, 140/80, 26, 95% RA Physical exam: 2 lacerations, 4-5 cm each, oozing mid axillary line, 9-10th intercostal space Left upper quadrant
- 3. Case #1 Physical exam Lungs slightly diminished on left 2+ pulses in extremities Abdomen: tense, firm, difficult to determine tenderness due to patient’s intoxication Back: no evidence of injury Treatment IV’s placed, NS bolus started FAST exam (focused abdominal sonography in trauma) performed by ER physician: questionable for fluid around liver
- 4. Stab wound to abdomen
- 6. Stab wound to abdomen Vitals stable after primary, secondary survey, airway intact Portable chest x-ray: small pneumothorax on left with small pleural effusion CT scan chest/abdomen/pelvis: 9th left rib fracture, hemothorax and 20% left pneumothorax, perforation of colon, pneumoperitoneum, hemoperitoneum Labs: Bicarbonate 21, glucose 108, creatinine 1.3, EtOH 148, HGB 12.6, UA neg, drug screen neg. INR normal. Decision to proceed to OR
- 7. Stab wound to abdomen
- 8. OR management Left chest tube placement for hemo/pneumothorax Exploratory laparotomy Stab wound through transverse colon-partial colectomy with anastamosis Control of mesenteric vascular bleeding Repair of left hemidiaphragm laceration Patient stabilized Post operative complication: Infection in pleural fluid (empyema) Leaking from colon anastomosis Back to OR for iliostomy Requiring TPN Massive transfusion
- 9. ATLS: stab wounds to abdomen Most commonly affected organs Liver (40%) Small bowel (30%) Diaphragm (30%) Colon (15%) Most commonly affected organs with GSW to abdomen Small bowel (50%) Colon (40%) Liver (30%) Abdominal vascular structures (25%)
- 10. OR or not?? History, knife length? Exam: signs of peritonitis? Vitals: Hypotensive? FAST exam positive? DPL (diagnostic peritoneal lavage) positive? Stable patient, CT findings? Stabbing to back/flank less likely to have to go to OR due to deep muscle presence.
- 11. OR guidelines 98% of GSW to abdomen require laparotomy 60% of stab wounds that penetrate anterior peritoneum have hypotension, peritonitis, or evisceration of omentum and/or small bowel that would necessitate going to OR for exploratory laparotomy.
- 12. Evisceration
- 13. Abdominal trauma: OR guidelines Blunt abdominal trauma with hypotension and positive FAST with evidence of intraperitoneal bleeding Blunt or penetrating abdominal trauma with positive DPL Hypotension with penetrating abdominal wound GSW transectiong peritoneal cavity or visceral/vascular retroperitoneum Evisceration Bleeding from stomach, rectum or GU tract from penetrating trauma
- 14. Abdominal trauma: OR guidelines Peritonitis Free air, rupture of hemidiaphragm CT positive for ruptured GI tract, intraperitoneal bladder injury, renal pedicle injury, or severe solid organ injury
- 15. Case #2 27 y/o male transferred from critical access hospital by Life net with left hand amputation Right hand dominant Amputation at wrist by wood cutter PMH/PSH: none. SH: positive for smoking VS : 151/98, 98.7, 94, 22, 96% on 2 liters nasal cannula IV present in right arm: 300 mcg Fentanyl, 4mg IV Zofran, 2 grams IV Ancef, Versed, 1 liter NS bolus Tetanus up to date Tourniquet removed in ER: no active bleeding Hand surgeon consult: To OR
- 16. Hand amputation
- 17. OR Reimplantation of hand Proximal row carpectomy Fasciotomies Reattachments of tendons, nerves, blood vessels Back to OR following day for left ulnar artery thrombosis. Hospitalized for 2 weeks
- 19. Amputations If transferring a patient with amputated part Stop bleeding Direct pressure is favored over tourniquet IV for pain control, antibiotics Tetanus updated if needed Judicious IVF (more IVF, more bleeding) Make NPO Send the detached part wrapped in gauze and “on ice”, not “in ice” Tissue survival time 6 hours if not cooled, 12 hours if cooled
- 20. Reattachment procedures Factors favoring successful reattachment Multiple fingers involved and/or thumb of dominant hand Younger patient without co-morbidities Nonsmoker Clean severed amputated part vs. tearing or crushed tissue
- 21. Steps in Reattachment X-raying and cleaning amputated part Debriding dead tissue Tagging nerves, blood vessels, and tendons with special surgical clips Trimming bone from amputated part, fixing it with K-wires, and stabilizing it to extremity Repair flexor and extensor tendons Repair lacerated arteries, veins and nerves Use of vein grafts for blood vessels that cannot be reattached Splint the extremity and elevate
- 22. Following reattachment Constant monitoring of tissue perfusion Medications may be used to increase blood flow, reduce anxiety, and for anti-coagulation Long term PT/OT Success Good nerve recovery >50% ROM of joint Acceptable cosmetic results Most likely will have cold intolerance in extremity
- 23. Complications Poor perfusion to reattached part Infection Need for further surgeries due to adhesions, scarring, infection, poor circulation
- 25. Case #3 31 y/o male transferred after fall from zip line, 41 feet into 6 feet of water, landing on buttocks. No LOC. Pt c/o left hand, wrist and buttock pain BLS transport with cervical and T/L/S immobilization PMH: Lumbar fracture with surgery after MVC rollover Lawnmower injury with traumatic right great toe amputation SH: positive for alcohol (8 beers)
- 26. Fall from height
- 27. Case #3 ED arrival 1730 128/90, 89, 16, 95% on RA GCS 15, Awake, Oriented x 3 Fully immobilized on backboard with cervical collar Chest wall abrasions on exam and pelvic tenderness but no instability Normal neurological and vascular exam No abdominal tenderness, FAST exam negative No cervical, TLS tenderness
- 28. Case #3 IVF, Morphine 4mg IV x 4, Fentanyl 100mcg, Zofran 4mg IV, tetanus updated, Rocephin 1 grams Xrays Left hand/wrist: positive for angulated and shortened distal radius fracture, comminuted distal phalanyx 4th finger Pelvis: superior right pubic rami fracture extending into right acetabulum Chest: patchy opacities middle lobe and left lung base Cervical/TLS spines: negative
- 31. Case #3 CT abdomen/pelvis: inferior left kidney laceration with hematoma surrounding, pubic rami fractures with adjacent hematomas, right medial acetabular fracture, fracture and left SI joint involving the lateral sacrum medial ilium CT chest: pulmonary contusions CT head: mildly displaced fracture inferolateral wall left maxillary sinus CT cervical: negative for fracture
- 33. Case #3 Left wrist fracture splinted 1900 decision to transfer to UNMC for trauma Life net unable to fly Ground transport arranged Ground transport cancelled as UNMC Life Net to fly 2015 Life net lands and pt transferred to UNMC (2 hours 45 minutes in ER) Decision to transfer Acetabular fracture Multi-organ system trauma
- 35. Case #3 UNMC follow up Pt went to surgery for ORIF of wrist fracture Admitted five days, discharged home Pelvic fractures non-operative Non-weight bearing right lower extremity and weight bearing as tolerated for left lower extremities for transfers only Wheelchair Also found to have Grade 1 spleen and liver lacerations managed non-operatively
- 36. Pelvic Fractures Types Closed fracture Lateral compression 60-70% frequency MVC Falls Internal rotation of involved hemipelvis Pelvic volume decreased so life-threatening hemorrhage not common Open book fracture Anterior-Posterior compression (15-20%) Auto-pedestrian collision Motorcycle crash Direct crush injury to pelvis Fall from > 12 feet
- 37. Pelvic fractures Open book pelvic fracture Disruption of symphysis pubis, tearing of posterior ligaments represented by sacroiliac fracture Opening of ring can lead to hemorrhage from pelvic venous complex and/or internal iliac artery Sheet or pelvic binder recommended for unstable pelvis fracture Vertical shear fracture 5-15% frequency High energy force in vertical plane Major pelvic instability Most likely from fall from significant height
- 38. Anatomy of pelvic bones
- 40. Open book pelvic fracture
- 41. Open book pelvic fracture
- 42. Vertical shear
- 43. Decision tree
- 45. Embolization of pelvic vessels Overall, 7-11% of pelvic fractures will require embolization Lateral compression fractures 2% need embolization due to arterial injury Open book (anterior-posterior compression), vertical shear or combined fractures 20% require embolization
- 46. Transfer to trauma hospital Significant resources required to care for patients with severe pelvic fractures Early consideration of transfer to trauma center is essential Trauma orthopedics Interventional radiology Multi-specialty as high likelihood of other injuries
- 47. Case #4 87 y/o female, chief complaint “weakness” brought to ER by family Symptoms x 3 days. Initially strained hip getting into car, left hip/leg pain Today, fell forward from swivel chair, caught arms and landed prone. No head injury LOC Feels dizzy and weak since, questionable syncope for several seconds at home today Difficulty with speech, slurred and expressive aphasia PMH: chronic atrial fibrillation, diabetes, HTN remote breast cancer
- 48. Case #4 Medications Coumadin among many others ER 130/66, 98, 70, 20, 100% RA c/o 10/10 hip/leg pain Exam No obvious head injury No cervical spine or TLS tenderness Lungs clear Heart irregular rhythm, rate normal 70, no murmur Extremities: mild left ankle tenderness, no swelling; left hip tender and pain with ROM of leg. No pain with internal/external rotation. Normal pulses
- 49. Case #4 Neurological: Awake and alert, sleepy but would wake easily Rectal: grossly guaiac positive Labs Hgb 8.8, Creat 1.6, Gluc 380, LFT’s 2-3 x normal, INR no clot detected (INR > 18) X-ray pelvis and left hip: normal X-ray left ankle: avulsion fracture off medial malleolus CT head: large left subdural hematoma with midline shift
- 52. Case #4 IV Morphine 2mg, Zofran 4mg given Pt with slurred speech, more sedate INR > 18, hgb 8.8 and grossly guaic pos stool (GI bleeding) Vitamin K 10mg IV FFP 4 units Transfer to neurosurgical center: UNMC
- 53. Burr Hole for evacuation
- 54. Burr Hole for evacuation
- 55. Craniotomy
- 56. Indications for Head CT in trauma Altered level of consciousness Neurological signs Severe headache, persistent vomiting, numbness, weakness on one side, slurred speech, facial droop Mental status difficult to evaluate Anesthesia, drug and alcohol intoxication, young children Low index of suspicion in elderly patients with minimal trauma and on anticoagulants
- 58. FRHS warfarin reversal protocol INR 5-9 without bleeding Vitamin K (Mephyton) 2.5mg PO once INR > 9 without bleeding Vitamin K (Mephyton) 5mg PO once Perioperative Non-Urgent Vitamin K 10mg IV once Life Threatening bleeding, add Kcentra INR 2 -<4: Kcentra (prothrombin complex concentrate) 25 units/kg IV once INR 4-6: Kcentra 35 units/kg IV once INR >6: Kcentra 50 units/kg IV once
- 59. KCentra Contains Vitamin K dependent coagulation factors II, VII, IX, and X (prothrombin complex) and the antithrombotic Protein C and Protein S. Made specifically to reverse warfarin in patient with acute major bleeding FDA approval randomized controlled trial FFP and Vitamin K Kcentra and Vitamin K
- 60. KCentra More likely to stop acute bleeding at 24 hour endpoint (72.4% of Kcentra vs 65% FFP) Faster reduction of INR (down 1.3 in 30 minutes in 62% of patients vs. 9.6% of FFP patients) Kcentra infusion produced a rapid and sustained increase in plasma levels of clotting factors within 30 minutes post treatment with 87% less volume than FFP. Common reactions: Headache, nausea/vomiting, arthralgia, hypotension. Most severe is thrombotic events (CVA,PE,DVT)
- 61. Case #4 outcome Transfer UNMC Neurosurgery consulted Reversal of warfarin coagulopathy Non-operative management of SDH MRI brain showed midbrain CVA Orthopedics Ankle fracture nonoperative GI consulted due to high bilirubin CT abdomen showed pancreatic mass, ERCP performed, biopsy done and stent placed Patient discharged to skilled nursing facility
- 63. Case #5 40 y/o female pedestrian struck Walking on side of county road, arguing with significant other. S.O. had parked car in middle of road. Car coming up behind them swerved to miss head on collision with parked car and hit patient. Pt was pinned under front passenger tire, laying prone. Right front tire was between her legs and left leg under engine block. Chest/abdomen was pinned under bumper. + LOC. Life net unable to fly to scene. BLS tiered with NFD ALS service.
- 64. Case #5 C-collar, backboard IV placed. Fentanyl given prehospital. VS: 122/76, 98, 23, 95% on RA Pt awake and alert, mildly confused. GCS 14 Exam: HEENT: no scalp swelling, laceration. Left periorbital bruising. PERRLA 3mm bilaterally. Airway intact. Teeth decayed Neck : in collar. NO c-spine tenderness
- 65. Case #5 Respiratory: lungs clear CV: RRR, Lungs clear bilaterally Abdomen: diffusely tender, no rebound/guarding Rectal: decreased tone, no blood MS: Midline and paraspinal lumbar tenderness, abrasion over lumbar spine. No pelvic tenderness Skin: 2cm left arm laceration, linear. 3rd degree linear burn on left lower extremity (2% BSA) Neuro: GCS 14. Alert. Disoriented to time. Short term memory loss. Both legs flaccid. Absent DTR’s patella. Sensory deficit to umbilicus.
- 66. Pedestrian Struck IVF, Fentanyl, zofran, tetanus, monitor FAST exam negative in ER Labs: drug screen pos meth, HGB normal X-ray C-spine lateral: neg to C7. posterior emphysema in neck Pelvis: no fracture Chest: Extensive emphysema in superior mediastinum, neck, chest wall bilaterally. No PTX appreciated Lumbar (one view, cross table lateral): no fracture
- 67. Pedestrian struck Consult to trauma center Suspected pulmonary contusions vs. pneumothorax Suspected spinal cord injury Suspected head injury Multi-organ system trauma plus third degree burn Patient transferred by Life Net to UNMC
- 71. Pedestrian struck Transfer to UNMC Findings: T 10/11 dislocation resulting in paraplegia Taken to OR for T8-L1 spinal fusion and open reduction of T 10/11 dislocation Bilateral rib fractures and pneumothoraces requiring chest tube placement 4th degree burns to left leg requiring debridement To follow up later regarding skin grafting Grade 1 thoracic aortic injury Nonoperative
- 72. Pedestrian struck Multiple facial fractures Nonoperative Left posterior acetabular fracture Nonoperative due to paralysis and non weight bearing Grade II spleen laceration and Grade III liver laceration, bilateral renal infarcts and adrenal hemorrhage Received multiple blood transfusions but remained stable thus nonoperative
- 73. Pedestrian struck Admitted 5/28-6/26/14 Transferred to Madonna for acute rehab
- 74. Thoracic aortic injury Blunt trauma Rapid deceleration by history Complete aortic transection = death at scene Partial transections Control blood pressure Identify other causes of hypotension/bleeding Surgical repair if actively bleeding
- 75. Chest x-ray findings Wide mediastinum (> 8 cm at aortic arch) Obliteration of aortic knob Deviation of trachea to right Depression of left mainstem bronchus Deviation of esophagus to right Left apical/ pleural cap Left hemothorax Fractures of 1st or 2nd rib or scapula
- 77. Suspicious for aortic injury
- 78. Aortic injury Chest x-ray findings 40-60% sensitive and specific Chest CT 97-100% sensitive 83-99% specific
- 79. Chest CT
- 80. Types of injury
- 81. Management Full thickness tear and are hemodynamically unstable Chest tube placement with large volume blood loss Over 1500 cc initially or 200 cc/hour x 2 hours of ongoing loss Indication for thoracotomy Evaluation for other injuries causing blood loss Abdominal or pelvic trauma Partial thickness tear Minor injuries such as small intimal flaps or small pseudoaneurysms are managed nonoperatively Blood pressure control < 120 systolic
- 83. References Encyclopedia of Surgery. Finger Reattachment. Web site Trauma.org: Permissive Hypotension. Barry Armstrong. 10/02 Trauma.org: Chest Trauma: Traumatic Aortic injury Advanced Trauma Life Support. American College of Surgeons. 9th edition. 2012