
Recommended
More Related Content
Similar to brachial plexus injury .pptx
Similar to brachial plexus injury .pptx (20)
More from Kollanur Charan
Recently uploaded
Recently uploaded (20)
brachial plexus injury .pptx
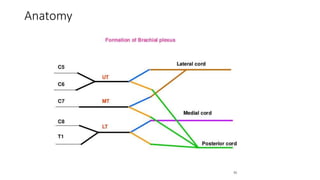
- 1. Anatomy
- 2. Surgical Management Of Traumatic And Congenital Brachial Plexus Injury
- 3. Indications and Timing • Closed injuries • Severe stretch injuries. • Grading motor or sensory function • Baseline set of electrodiagnostic studies at 3 or 4 weeks after injury • Followed for 3 to 4 months • Operated if there is no significant improvement in function • Those capable of recovery may be prematurely resected and replaced by grafts • Good range of motion while waiting .
- 4. • OPEN INJURIES • Clean and sharp lacerations, the plexus elements are usually repaired acutely, within 72 hours • If the laceration is jagged, with the nerve ends contused and edematous, suture the ends surrounding muscle to prevent it from retracting and shrinking. • The definitive repair is delayed for 3 weeks in order to allow the longitudinal extent of the injury to be fully delineated.
- 5. • Gunshot injuries • Low-velocity civilian gunshot , small shock wave ,transient neurologic deficit • Observed for 3 to 4 months before surgical exploration • May have vascular injuries. • Transection major vessel, pseudoaneurysms or arteriovenous fistulas • Compress the plexus, produce progressive loss of function and pain.
- 6. • Iatrogenic plexus injuries • Operations or medical maneuvers around neck and shoulder • Mechanisms - scalpel, scissors, or rongeur • Crush injury caused by a hemostat or a retractor • Traction injury from hyperabduction of the shoulder • Same criteria to select patients for surgery • Sharply divided plexus , primary end-to-end repair. • Bluntly transected, the contused stumps tacked to fascia • Secondary delayed repair.
- 7. Goals Of Surgery • Restore shoulder abduction, external rotation, elbow flexion, and forearm supination. • Hold a food tray, bring hand to mouth, push doors open while carrying.
- 8. Operative technique • Positioned supine • Roll under ipsilateral shoulder • Head turned to opposite side. • Ipsilateral leg should be prepped for harvesting the sural nerve • Supraclavicular exploration • A transverse incision 2 cm above and parallel to clavicle, at base of posterior triangle
- 9. • Infraclavicular exploration • Curvilinear hockey stick incision is made over the deltopectoral groove • Overlying soft tissues are dissected • Elements are dissected in a 360-degree fashion to free them from the surrounding structures • NAPs are measured by stimulating the proximal spinal nerve and recording from distal trunks • If NAPs are positive, small in amplitude, slow in conduction then element is regenerating, therefore is not sectioned.
- 10. Types of procedures 1. Neurolysis. • Exploration and dissection of plexus elements in circumferential, 360-deg fashion. • No interference if found regenerating (positive nerve action potentials) 2. End-to-end repair • When the nerve ends can be reapproximated without tension. • Early exploration of sharp penetrating injuries (within 72 hours).
- 11. 3. Graft repair. • Used to bridge the gap between two unscarred nerve ends • Provide conduit for regenerating axons. e.g sural nerve 4. Neurotization (nerve transfers). • Is the repair of distal denervated nerve element • Using proximal foreign nerve as the donor • To reinnervate and restore function to a denervated end-organ. 5. Salvage procedures • Tendon and free muscle transfers.
- 12. Complications • Wound complications seroma, lymph collections, and infections. • Injury to phrenic and the musculocutaneous nerves • Risk of vascular injury vertebral artery, the subclavian artery and vein and the circumflex humeral artery. • Future directions • Stem cells and growth factors may augment nerve injury repair and accelerate nerve regeneration.
- 15. Birth-related peripheral nerve injury (BRPNI) • Caused by traction during delivery pattern concerns infants, usually with low birth weight, born in a breech position. • There is an ongoing debate whether the BRPNI can be prevented and whether the obstetrician can be held responsible.
- 16. Conservative Treatment • For the First Few Months of Life • We recommend frequent mobilization of the joints from the beginning to prevent formation of joint contractures. • Joint contracture formation, might be detrimental to final functional outcome.
- 17. Selecting patients for surgery • Restricted to cases in which spontaneous restoration will not occur • Physiotherapy from 1 month age • Operative intervention - no spontaneous recovery of shoulder external rotation and elbow flexion and forearm supination • 3 to 4 months of age. • Before 7 months.
- 18. Surgical procedure • Supraclavicular exposure • General anesthesia without muscle-blocking agents. • Supraclavicular brachial plexus is exposed in posterior triangle. • Supine, head turd toward the opposite, neck extension • Affected arm lies at 45 degrees • A linear incision 1.5 cm above and parallel to the clavicle. • Soft tissue dissected is performed.
- 19. • External jugular vein, spinal accessory nerve • Supraclavicular nerves are followed until C4 spinal nerve root. • From the C4 spinal nerve root, a branch from this nerve can be followed to the phrenic nerve • One should preserve or ligate the thoracic duct to avoid leakage of chyle. • Vertebral artery, runs unprotected at the roots C8–T1 before it enters in the lateral mass of C7. • Infraclavicular exposure infraclavicular extension of the lesion in brpni is quite rare.
- 20. • Endoscopic assistance for neurolysis of the sural nerve. B, The leg is positioned vertically with the help of an iron bar and tape. C, View from the surgeon’s position. The sural nerve can be seen in the center of the monitor. D, Detailed view of the image on the monitor. The sural nerve is dissected free with the aid of a small hook and fine bayonet scissors. E, The end result after harvesting the sural nerve using three short incisions; the nerve has been cut proximally.
- 21. Postoperative care • Upper body placed in a prefabricated cast • Limit movement of head and affected arm for 2 wks. • Clinical examinations 6-month intervals. • Results • n = 86 • Only 20% gained true glenohumeral external rotation • 87% could reach their mouth • 75% could reach the back of head. • Great ability of the infants to compensate limited true external rotation by thoracoscapular movements. • Biceps muscle force against gravity was gained in 92% of patients.
- 22. • Thank you