2. RENIN-ANGIOTENSIN (RAS) SYSTEM –
RECALL PHYSIOLOGY
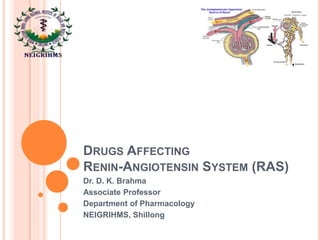
Angiotensin – II is an
octapeptide generated in
plasma from precursor
plasma α2 globulin –
involved in electrolyte, blood
volume and pressure
homeostasis
Enzyme Renin generates
inactive Angiotensin – I from
plasma protein)
Angiotensin-I is rapidly
converted to Angiotensin-II
(A-II) by Angiotensin
Converting Enzyme (ACE)
(present in luminal surface
of vascular endothelium)
Essentials of Medical pharmacology by KD Tripathi – 7th
Edition, JAYPEE, 2013
3. TYPES – CIRCULATING RAS AND TISSUE RAS
Circulating RAS: Renin is the rate limiting factor of Ang-II release
Plasma t1/2 of Renin is 15 minutes
Ang-I is less potent (1/100th) than of Ang-II
Ang-I is rapidly converted to Ang-II by ACE (in vascular endothelium- mainly
lungs)
Ang-II half life is 1 minute only
Degradation product is Ang-III (heptapeptide) - 2-10 times less potent than
Ang-II
Both Ang-II and An-III stimulates Aldosterone secretion from Adrenal Cortex
(equipotent)
Ang-IV – different from all – mainly CNS action via AT4 receptor
Tissue RAS:
Blood vessels capture Renin and Angiotensinogen from circulation – produce
Ang-II (Extrinsic local RAS) – on cell surface – local response
Many tissues also - Heart, brain, kidneys, adrenals capture Renin and
Angiotensinogen to produce intracellularly Ang-II (Intrinsic local RAS) -
Important in these organs – regulates organ function, cell growth/death
4. TISSUE RAS - PRORENIN AND (PRO) RENIN
RECEPTOR
JG cells and RAS expressing
tissues/organs synthesize pre-
prorenin
In response to stimuli Prorenin
and renin secreted
Prorenin activated –
enzymatically (irreversible)
Also non-enzymatically
(reversible) – binding to (Pro)
renin receptor (PRR) – exposes
catalytic domain of Prorenin -
also binding to PRR Renin
increases its catalytic activity –
ENERGY BOOSTER
Non enzymatic activation has
major Role in local RAS via
Ang-II – heart, BV, kidneys,
brain, eye and liver
Essentials of Medical pharmacology by KD Tripathi –
7th Edition, JAYPEE, 2013
5. THE PATHWAYS
Ang II dependent pathway –
activation of prorenin/renin generates
Ang I and then Ang II by ACE
Ang II independent pathway – binding
of prorenin/renin to PRR on cell
surface – direct activation of MAP
kinase, PAI-1, JAK-STAT pathway,
transcription factor, protooncegenes
etc.
Alternative pathway: Small amount -
Ang II and Ang II produced by
cathepsin, chymase etc.
Other angiotensins: Ang IV – acts via
inhibiting AT4 receptor or Insulin
regulated aminopeptidase (IRAP)
Ang (1-7): Produced from Ang I or
Ang II – by ACE-2 – action opposite
of Ang II ACEIs enhance action
Essentials of Medical pharmacology by KD Tripathi
– 7th Edition, JAYPEE, 2013
6. ACTIONS OF ANGIOTENSIN-II - CVS
Powerful vasoconstrictor particularly arteriolar and
venular
direct action
release of Adr/NA release (adrenal and adrenergic nerve
endings)
increased Central sympathetic outflow
Promotes movement of fluid from vascular to
extravascular
Less prominent in cerebral, skeletal, pulmonary and
coronary
Overall Effect – Pressor effect (Rise in Blood
pressure)
More potent vasopressor agent than NA –promotes
Na+ and water reabsorption and no tachyphylaxis
Cardiac action:
Increases myocardial force of contraction (Ca++ influx
promotion)
Increases heart rate by sympathetic activity - but reflex
bradycardia occurs
Cardiac output is reduced
Cardiac work increased (increased Peripheral resistance)
7. ANG-II ON CHRONIC BASIS – ILL EFFECT
Directly: Induces hypertrophy, hyperplesia and
increased cellular matrix of myocardium and vascular
smooth muscles – by direct cellular effects involving
proto-oncogens and transcription of growth factors
Indirectly: Volume overload and increased t.p.r in heart
and blood vessels
Ventricular Hypertrophy and Remodeling (abnormal redistribution
of muscle mass)
Long standing hypertension – increases vessel wall
thickness and Ventricular hypertrophy
Myocardial infarction – fibrosis and dilatation in
infarcted area and hypertrophy of non-infarcted area of
ventricles
CHF – progressive fibrotic changes and myocyte death
Risk of increased CVS related morbidity and mortality
ACE inhibitors reverse cardiac and vascular
hypertrophy and remodeling
9. OTHER ACTIONS OF
ANGIOTENSIN-II – CONTD.
Adrenal cortex: Enhances the synthesis and release of
Aldosterone
In distal tubule Na+ reabsorption and K+/H+ excretion
At lower conc. than vasoconstrictor effect
Kidney: Enhancement of Na+/H+ exchange in proximal
tubule – increased Na+, Cl- and HCO3 reabsorption
Also reduces renal blood flow and GFR - promotes Na+ and
water retention
CNS: Drinking behaviour and ADH release
Peripheral sympathetic action: Stimulates adrenal
medulla to secrete Adr and also releases NA from
autononic ganglia
10. AT-II – PATHOPHYSIOLOGICAL ROLES
1. Mineraocorticoid secretion – Physiological stimulus of
Aldosterone secretion
2. Electrolyte, blood volume and pressure homeostasis: Renin is
released when there is change in blood volume or pressure or
decreased Na+ content:
I. Reduction in tension in afferent gromerulus - Intrarenal Baroreceeptor
Pathway (PG) activation – PG production - Renin release
II. Low Low Na+ and Cl- conc. in tubular fluid – macula densa pathway – COX-2
and nNOS are induced – release of PGE2 and PGI2 – more renin release
III. Baroreceptor stimulation increases sympathetic impulse – via β-1 pathway –
renin release
Renin release – increased Ang-II production – acute rise in BP
direcytly acting by vasoconstriction and indirectly, increased Na+
and water reabsorption
Long-loop negative feedback mechanism: Rise in BP – decreased
Renin release
Short-loop -ve feedback mechanism: A-II also formed locally in the
Kidneys
Activation of AT1 receptor in JG cells – inhibition of Renin release
Overall - Long term stabilization of BP – independent of salt and water
intake
12. ANG-II ROLES – CONTD.
Pharmacological implications:
Drugs Increasing Renin release:
ACE inhibitors and AT1 receptor antagonists enhance
Renin release
Vasodilators and diuretics stimulate Renin release
Loop diuretics increase renin release
Decrease in Renin release:
Beta blockers and central sympatholytics
NSAIDs and selective COX-2 inhibitors decrease Renin
release
13. ROLE OF AT-II – CONTD.
3. Hypertension development
• Renovascular hypertension – PRA activity
• Essential hypertension
• Pre-eclampsia – AT1 receptor agonist antibodies
4. Secondary hyperaldosteronism
Inhibitors of RAS
Sympathetic blockade
ACE inhibitors
AT1 receptor antagonists
Aldosterone antagonists
Renin inhibitory peptides and Renin specific antibodies
14. ANGIOTENSIN RECEPTORS
2 (two) subtypes: AT1 and AT2 (opposite effects)
– most of known Physiologic effects are via AT1
Both are GPCR
Utilizes various pathways for different tissues
PLC-IP3/DAG: AT1 utilizes pathway for vascular
smooth muscles by MLCK
Membrane Ca++ release: aldosterone synthesis,
cardiac inotropy, CA release - ganglia/adrenal
medulla action etc.
Adenylyl cyclase: in liver and kidney (AT1)
Intrarenal homeostatic action: Phospholipase A2
15. ACE INHIBITORS AND ARBS - DRUGS
ACE Inhibitors:
Captopril, enalapril,
lisinopril, perindopril,
fosinopril, benazepril
ramipril and imidapril,
Benazepril etc.
ARBs: Losartan,
candesartan,
irbesartan, valsartan
and telmisartan
16. CAPTOPRIL …… TEPROTIDE
Surrogate of Proline – abolishes only Ang-I actions, not on Ang-II
ACE – non-specific enzyme– splits off dipeptidyl segment - bradykinin,
substance P, natural stem cell regulating peptide
• Captopril increases plasma kinin levels – potentiate hypotensive action
of bradykinin - overall hypotensive effects
However, increased kinin level by Captopril - no role on long term regulation of BP –
Kinins play minor role in BP regulation and Kininase I
But increased kinins – PG synthesis – cough and angioedema
Rise in stem cell regulator peptide - cardioprotective
But, BP lowering is not long term - depends on Na+ status and level of
RAS
In normotensives:
With normal Na+ level – fall in BP is minimal
But restriction in salt or diuretics - more fall in BP
In CHF (increased renin) – marked fall in BP
Most effective greater fall in BP: Renovascular and malignant
hypertension
Essential hypertension: 20% hyperactive RAS and 60% normal in RAS
Contributes to 80% of maintainence of tone – lowers BP
17. CAPTOPRIL – CONTD.
ACEI – feedback increase in Renin release – but, ACE blocked –
Ang I converted to Ang (1-7) by ACE-2 ---BP lowering
Actions:
Decrease in peripheral Resistance
Arteriolar dilatation and compliance of larger arteries increased
Fall in Systolic and Diastolic BP - No effect on Cardiac output
No reflex sympathetic stimulation – Can be used safely in IHD patients
Little dilatation of capacitance vessels
Minimal Postural hypotension
Renal blood flow is maintained – Ang-II constricts them
Cerebral and coronary blood flow – not affected
Pharmacokinetics:
• 70% absorbed, partly metabolized and partly excreted unchanged in
urine
• Food interferes absorption
• T1/2 = 2 Hrs (6-12 Hrs)
18. CAPTOPRIL – ADVERSE EFFECTS
1. Cough – persistent brassy cough in 20% cases – inhibition
of bradykinin and substance P breakdown in lungs
2. Hypotension – initial sharp fall in BP – diuretics + CHF
3. Hyperkalemia in renal failure patients with K+ sparing
diuretics, NSAID and beta blockers (routine check of K+
level)
4. Acute renal failure: CHF and bilateral renal artery stenosis
5. Angioedema: swelling of lips, mouth, nose etc. – 0.5%
6. Rashes, urticaria etc. – 1 – 4%
7. Dysgeusia: loss or alteration of taste
8. Foetopathic: hypoplasia of organs, growth retardation etc.
9. Neutripenia and proteinuria
10. Acute Renal Failure – in bilateral renal artery stenosis
Contraindications: Pregnancy, bilateral renal artery stenosis,
hypersensitivity and hyperkalaemia
19. ACE INHIBITORS - ENALAPRIL
It’s a prodrug – converted to enalaprilate
Not used orally – poor absorption
Advantages over captopril:
Longer half life – OD (5-20 mg OD)
Absorption not affected by food
Rash and loss of taste are less frequent
Longer onset of action
Less side effects
20. ACE INHIBITORS – LISINOPRIL
(LIPRIL/LISTRIL)
It’s a lysine derivative
Not a prodrug
Slow oral absorption – less chance of 1st dose
phenomenon
Absorption not affected by food and not
metabolized – excrete unchanged in urine
Long duration of action – single daily dose
Doses: available as 1.25, 2.5, 5, 10 and 20 mg tab
– start with low dose
21. ACE INHIBITORS – RAMIPRIL (CARDACE)
It’s a popular ACEI now - long acting and extensive
tissue distribution
It is also a prodrug with long half life
Tissue specific – Protective of heart and kidney
Uses: Diabetes with hypertension, CHF, AMI and cardio
protective in angina pectoris
Blacks in USA are resistant to Ramipril – addition of
diuretics help
Dose: Start with low dose; 2.5 to 10 mg daily
EBM Reports: 1) improves mortality rate in early AMI
cases 2) reduces the chance of development of AMI 3)
reduces the chances of development of nephropathy
etc. (1.25, 2.55 … 10 mg caps)
22. USES - ACEI AND HYPERTENSION
1st line of Drug: advantages renovascular and
resistant
No postural hypotension or electrolyte imbalance (no
fatigue or weakness)
Safe in asthmatics and diabetics
Prevention of secondary hyperaldosteronism and K+
loss (diuretics)
Renal perfusion well maintained
Reverse the ventricular hypertrophy and increase in
lumen size of vessel
No hyperuraecemia or deleterious effect on plasma
lipid profile
No rebound hypertension
Minimal worsening of quality of life – general
wellbeing, sleep and work performance etc.
23. ACE INHIBITORS – USES
Congestive Heart Failure:
Reduction in preload and afterload
Some benefits - Reduction in pulmonary artery pressure, right atrial
pressure, systemic vascular resistance
Improved Renal perfusion (Na+ and water excretion)
CO and stroke volume increases – with reduced heart rate (less cardiac
work)
1st line of drug with beta-blocker and diuretics in all cases (digitalis ?)
Myocardial Infarction: 0 – 6 weeks
Reduces mortality
Also reduces recurrent MI
Extension of therapy – in CHF patients
Prophylaxis of high CVS risk subjects: Ramipril – post MI,
diabetes etc.
Diabetic Nephropathy and non-diabetic nephropathy – reduce
albuminuria (both type 1 and 2) – higher creatinine clearance
Better haemodynamic and prevention of mesangial growth
Schleroderma crisis: Rise in BP and deteriorating renal function
(Ang –II)
25. ANGIOTENSIN RECEPTORS
2 (two) subtypes: AT1 and AT2 (opposite effects) –
most of known Physiologic effects are via AT1
Both are GPCR
AT1 utilizes various pathways for different tissues
Ang III also activates AT1 and AT2 – but weak
Also Ang IV and Ang (1-7) – uses AT4 and Mas
AT2 receptors – expressed in foetus – high quantity
Also in vascular endothelium, adrenal medulla, kidney and
brain areas
NO-dependent vasodilatation, apoptosis, myocardial
fibrosis, inhibits cell proliferation and lower BP
26. LOSARTAN
Competitive antagonist and inverse agonist of AT1
receptor – 10,000 times for AT1
Does not interfere with other receptors except TXA2
– platelet antiaggregatory
Blocks all the actions of Ang-II - - - vasoconstriction,
sympathetic stimulation, aldosterone release and
renal actions of salt and water reabsorption, growth
promoting effects in heart and blood vessels and
central action (thurst) etc.
No inhibition of ACE
27. LOSARTAN
Theoretical superiority over ACEIs:
Cough is rare – no interference with bradykinin, Substance
P and other ACE substrates
Complete inhibition of AT1 – alternative pathway remains
for ACEIs
Result in indirect activation of AT2 – vasodilatation
Little increase in Ang (1-7) - vasodilatation
Clinical benefit of ARBs over ACEIs – not known
However, losartan decreases BP in hypertensive which is for
long period (24 Hrs) –
Heart rate remains unchanged and cvs reflxes are not
interfered
No significant effect in plasma lipid profile, insulin
sensitivity and carbohydrate tolerance etc.
Mild uricosuric effect
28. LOSARTAN
Pharmacokinetic:
Absorption not affected by food but unlike ACEIs its
bioavailability is low (30 – 40%)
High first pass metabolism
Carboxylated to active metabolite E3174
Highly bound to plasma protein
Do not enter brain
No dose adjustment in renal insufficiency
Adverse effects:
Foetopathic like ACEIs – not to be
administered in pregnancy
Rare 1st dose effect hypotension & cough
Low dysgeusia and dry cough
Lower incidence of angioedema
Available as 25 and 50 mg tablets
29. LOSARTAN/ARBS - USES
Same range of clinical utility with ACE inhibitors
1. Hypertension: Commonly prescribed now than ACEIs
– better than beta-blockers in reducing stroke
2. CHF: Superiority over ACEIs uncertain
3. Myocardial Infarction – ACEIs preferred
4. Diabetic Nephropathy
5. Combination with ACEIs – theoretical
• ARBs: Ang II generated in local tissues by non-ACE
mechanism with ACEIs - ARBs block
• ACEIs: vasodilatation due to bradykinin & Ang (1-7) – not
produced by ARBs
• Increase in Ang II by ARBs – blocked by ACEIs
• Increase in AT2 action with ARBs can be prevented by
ACEIs
30. DIRECT RENIN INHIBITOR - ALISKIREN
Nonpeptide – competitive blocker of catalytic site of Renin –
Ang-I not produced from Angiotensinogen
Concentration of Renin increases, but PRA decreased
Pharmacological actions:
Causes fall in BP – Na+ depleted states more
Plasma aldosterone level decreased – K+ retention occurs
Equivalent to ACEIs and ARBs in reducing BP – combination of all 3
- greater fall in BP
Renoprotective – hypertension and DM – being evaluated
Used as alternative – do not respond/tolerate 1st line
Kinetics: Orally effective – low bioavailability (p-glycoprotein) –
half life = > 24 hours
ADRs: Dyspepsia, loose motions, headache, dizziness – lesss
rash, hypotension, hyperkalaemia, cough, angioedema etc.
Contraindication - Pregnancy
31. MUST KNOW
Drugs - ACEIs and ARBs
ACEIs – Pharmacological actions and the common
ADRs
Therapeutic uses of ACEIs
Captopril, Ramipril, Losartan
Role of ACEIs/ARBs in the management of
Hypertension, CHF and MI
32. THANK YOU
Ace in Heart
Diseases
Trying to be
Healthy
ACEIs and ARBs