1. Discussion
Pityriasis
lichenodes
(PL)
is
a
rare
idiopathic
skin
condi5on
that
commonly
affects
gene5cally
suscep5ble
male
children
(19%-‐38%),
with
peak
incidences
at
the
age
of
5
and
age
of
10.
Under
the
umbrella
term
of
PL,
there
are
various
subtypes
of
the
disorder:
acute
(PLA),
chronic
(PLC),
and
the
febrile
disorder,
Mucha-‐
Habermanns
disease.1
The
acute
form
is
characterized
as
erup5ons
of
small
2-‐3
mm
reddish-‐brown
clusters
of
papules
on
the
skin,
which
fill
with
pus
and
blood
and
cause
itching
and
burning;
and
in
severe
cases
begin
to
ulcerate.
PLC
will
oSen
appear
with
small
scaling
papules
that
upon
resolu5on
will
leave
hypopigmenta5on.
Simultaneous
systemic
symptoms
like
fever,
lymphadenopathy
and
necro5zing
papules
will
occur
in
Mucha-‐
Habermanns
disease.2
Diagnosis
is
oSen
difficult
because
of
the
lack
of
clinical
guidelines
and
its
some5mes-‐similar
presenta5on
to
atopic
derma55s.
Currently,
diagnosis
relies
on
clinical
presenta5on,
ruling
out
of
other
disorders
and
histological
examina5on.
Although
the
e5ology
and
pathology
of
PL
remains
unknown,
it
is
hypothesized
that
PL
is
a
atypical
immune
response
triggered
by
an
infec5ous
agent
because
the
symptoms
and
papules
generally
improve
aSer
an5bio5c
therapy.3
Current
standard
of
treatment
of
a
pa5ent
with
PL
is
oral
an5bio5c
(tetracycline
or
erythromycin),
topical
cor5costeroid,
and
light
therapy.
The
results
have
varying
degrees
of
success
and
occasionally
resolve
on
its
own
aSer
several
weeks
to
months.4
Background
Classic Chinese Herbal Formulas for the Treatment of
Pityriasis Lichenodes: A Case Study of a 7 Year Old Boy
Judith Miller, MAOM (c)
San Hong Hwang, MD (Taiwan), OMD
A
7
year-‐old
boy
with
a
mild
form
of
PL
was
brought
to
the
SCU
Health
System
in
Whi[er,
CA
in
September
2013.
The
boy
is
a
Caucasian
of
Moroccan
and
Cuban
descent.
The
onset
of
the
skin
rash
began
during
a
family
vaca5on
to
Hawaii
in
June
2013.
The
small,
red,
itchy
papules
ini5ally
arose
on
his
stomach
and
then
progressed
to
his
limbs
and
face.
From
June
to
August
the
pa5ent
was
ini5ally
diagnosed
with
a
viral
infec5on,
insect
bites
and
scabies.
During
this
5me
he
was
prescribed
200mg
of
liquid-‐oral
erythromycin,
which
did
not
alleviate
his
symptoms
or
improve
the
skin
condi5on.
He
was
eventually
diagnosed
with
PL
aSer
a
histological
exam
in
September
2013.
He
has
no
prior
history
of
any
skin
condi5ons,
but
his
mother
and
other
immediate
family
members
have
a
history
of
psoriasis
and
eczema.
Case
presenta3on
Diagnosis
and
Treatment
At
the
5me
of
presenta5on,
the
pa5ent
had
several
2-‐3mm
bright
red,
non-‐ulcera5ng
papules
covering
his
en5re
body
and
face
associated
with
severe
itching
at
night.
No
history
of
any
discharge
was
reported.
His
vitals
and
other
physical
exam
findings
were
within
normal
limits.
His
mother
reported
that
the
boy
started
his
second
course
of
erythromycin
at
the
same
5me
when
he
reported
to
our
clinic.
His
tongue
was
found
to
be
red
with
prickles
with
a
greasy
white
coat,
and
his
pulse
was
slightly
slippery.
His
TCM
diagnosis
was
determined
as
an
invasion
of
wind-‐damp
and
fire-‐toxin.
He
was
prescribed:
Huáng
Lián
Jiě
Du
Tāng
(Cop4s
Decoc4on
to
Resolve
Toxicity)
and
Xiāo
Fēng
Sān
(Eliminate
Wind
Powder
from
Orthodox
Lineage)
in
granule
form
made
by
TCM
Zone®.
He
was
given
700mg
BID.
Yù
Píng
Fēng
Săn
(Jade
Windscreen
Powder)
was
subs5tuted
for
Xiao
Feng
San
(Eliminate
Wind
Powder
from
Orthodox
Lineage)
aSer
two
weeks
based
on
his
improved
skin
condi5on.
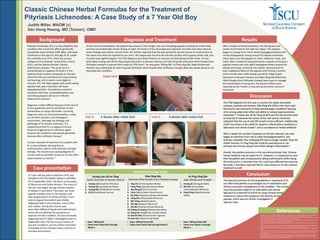
Ini3al
Visit
Visit
3:
2
Weeks
A>er
Ini3al
Visit
Visit
5:
4
Weeks
A>er
Ini3al
Visit
Herbal
Formulas
Used
Huáng
Lián
Jiě
Du
Tāng
Cop4s
Decoc4on
to
Resolve
Toxicity
Xiāo
Fēng
Sān
Eliminate
Wind
Powder
from
Orthodox
Lineage
Yù
Píng
Fēng
Săn
Jade
Windscreen
Powder
1. Huáng
Lián
(Cop5dis
Rhizoma)
2. Huáng
Qín
(Scutellariae
Radix)
3. Huáng
Băi
(Phellodendri
Cortex)
4. Zhī
Zĭ
(Gardeniae
Fructus)
1. Jīng
Jiè
(Schizonepetae
Herba)
2. Fáng
Fēng
(Saposhnikoviae
Radix)
3. Niú
Bàng
Zĭ
(Arc5i
Fructus)
4. Chán
Tuì
(Cicadae
Periostracum)
5. Kŭ
Shēn
(Sophorae
flavescen4s
Radix)
6. Cāng
Zhú
(Atractylodis
Rhizoma)
7. Mù
Tōng
(Akebiae
Caulis)
8. Shí
Gāo
(Gypsum
fibrosum)
9. Zhī
Mŭ
(Anemarrhenae
Rhizoma)
10. Shēng
Dì
Huáng
(Rehmanniae
Radix)
11. Dāng
Guī
(Angelicase
sinensis
Radix)
12. Hēi
Zhī
Má
(Sesami
Semen
nigrum)
13. Gān
Căo
(Glycyrrhizae
Radix)
1. Huáng
Qĭ
(Astragali
Radix)
2. Bái
Zhú
(Atractylodis
macrocephalae
Rhizoma)
3. Fáng
Fēng
(Saposhnikoviae
Radix)
• Dose:
700mg
BID
• Taken
from
Ini3al
Visit
through
Week
4
• Dose:
700mg
Packet
BID
• Taken
from
Ini3al
Visit
through
Week
2
• Dose:
700mg
Packet
BID
• Taken
from
Week
3
through
Week
4
ASer
2
weeks
of
herbal
treatment,
the
itching
was
less
severe
and
limited
to
the
right
hip
region.
The
papules
began
to
change
from
red
to
white
(hypopigmenta5on)
and
mostly
disappeared,
except
around
his
elbows
and
knees.
There
were
very
few
papules
on
chest,
abdomen,
back,
and
limbs.
ASer
4
weeks
of
taking
the
herbs,
majority
of
the
boy’s
papules
healed
and
only
slight
hypopigmenta5on
around
the
elbows
and
knees
remained.
His
mother
reported
that
he
had
2
addi5onal
flares
of
red
papules
with
itching
2
months
and
6
months
later.
Both
Huáng
Lián
Jiě
Du
Tāng
(Cop4s
Decoc4on
to
Resolve
Toxicity)
and
Xiāo
Fēng
Sān
(Eliminate
Wind
Powder
from
Orthodox
Lineage)
were
used
to
manage
the
exacerba5on
of
symptoms.
No
adverse
effects
were
reported
by
the
mother
or
boy
during
the
en5re
course
of
treatment.
The
TCM
diagnosis
for
this
case
is
common
for
atopic
derma55s,
ur5caria,
psoriasis
and
eczema.
Xiāo
Fēng
Sān
(XFS)
is
the
most
used
formula
for
the
treatment
of
these
dermatologic
condi5ons5
because
of
its
strong
an5pruri5c
effect
and
ability
to
reduce
hypersensi5vity
responses.6,7
Huáng
Lián
Jiě
Du
Tāng
(HLJDT)
was
the
key
formula
used
to
treat
the
PL
because
the
nature
of
the
rash
and
its
chronicity
indicated
that
the
use
of
only
XFS
would
not
be
sufficient.
Addi5onally,
HLJDT
has
shown
to
be
useful
for
systemic
inflammatory
condi5ons
in
laboratory
and
clinical
studies7,
and
is
considered
an
herbal
an5bio5c.
ASer
2
weeks
the
number
of
papules
on
the
skin
reduced,
the
color
began
to
transform
from
red
to
white
(hypopigmenta5on),
and
itchiness
subsided;
thus
indica5ng
XFS
was
no
longer
needed.
Now
the
milder
formula,
Yù
Píng
Fēng
Săn
could
be
used
because
it
can
enhance
the
immune
system
and
inhibit
allergic
inflamma5on.9
Overall,
the
posi5ve
outcome
in
this
case
demonstrates
that
Chinese
herbal
medicine
may
be
useful
for
PL.
However,
it
is
important
to
note
that
the
pa5ent
was
simultaneously
taking
erythromycin
while
taking
the
herbs
and
it
is
unknown
how
this
could
have
affected
the
outcome.
Secondly,
it
has
been
reported
that
PL
may
resolve
on
its
own
without
treatment
as
well.
The
obscurity
and
lack
of
clinical
guidelines
in
treatment
of
PL
can
oSen
lead
pa5ents
to
prolonged
use
of
medica5ons
and
without
successful
management
of
the
condi5on.
The
current
case
may
provide
insight
to
an
alterna5ve
and
natural
approach
to
treatment
of
PLEVA
by
using
Chinese
herbal
medicine
to
reduce
the
symptoms
and
severity
of
the
papules,
which
warrant
further
inves5ga5on
in
rigorous
trials.
Conclusion
References
Results
1. Markus
JR,
Carvalho
VO,
Lima
MN,
Abagge
KT,
Nascimento
A,
Werner
B.
The
relevance
of
recognizing
clinical
and
morphologic
features
of
pityriasis
lichenoides:
clinicopathological
study
of
29
cases.
Dermatol.
Pract.
Concept.
2013;3(4):7-‐10.
2. 2.
Brazzelli
V,
Carugno
A,
Rive[
N,
Cananzi
R,
Barrusco[
S,
Borroni
G.
Narrowband
UVB
phototherapy
for
pediatric
generalized
pityriasis
lichenoides.
Photodermatol.
Photoimmunol.
Photomed.
2013;29(6):330-‐333.
3. Pereira
N,
Brinca
A,
Manuel
Brites
M,
José
Julião
M,
Tellechea
O,
Gonçalo
M.
Pityriasis
lichenoides
et
varioliformis
acuta:
case
report
and
review
of
the
literature.
Case
Rep.
Dermatol.
2012;4(1):61-‐65.
4. Hapa
A,
Ersoy-‐Evans
S,
Karaduman
A.
Childhood
pityriasis
lichenoides
and
oral
erythromycin.
Pediatr.
Dermatol.
2012;29(6):
719-‐724.
5. Lin
J-‐F,
Liu
P-‐H,
Huang
T-‐P,
et
al.
Characteris5cs
and
prescrip5on
pazerns
of
tradi5onal
Chinese
medicine
in
atopic
derma55s
pa5ents:
ten-‐year
experiences
at
a
medical
center
in
Taiwan.
Complement.
Ther.
Med.
2014;22(1):141-‐147.
6. Chang
Y-‐T,
Shen
J-‐J,
Wong
W-‐R,
Yen
H-‐R.
Alterna5ve
therapy
for
autosensi5za5on
derma55s.
Chang
Gung
Med.
J.
2009;32(6):
668-‐673.
7. Cheng
H-‐M,
Chiang
L-‐C,
Jan
Y-‐M,
Chen
G-‐W,
Li
T-‐C.
The
efficacy
and
safety
of
a
Chinese
herbal
product
(Xiao-‐Feng-‐San)
for
the
treatment
of
refractory
atopic
derma55s:
a
randomized,
double-‐blind,
placebo-‐controlled
trial.
Int.
Arch.
Allergy
Immunol.
2011;155(2):141-‐148.
8. Li
L,
Zeng
H,
Shan
L,
et
al.
The
different
inhibitory
effects
of
Huang-‐Lian-‐Jie-‐Du-‐Tang
on
cyclooxygenase
2
and
5-‐lipoxygenase.
J.
Ethnopharmacol.
2012;143(2):732-‐739.
9.
Lau
TF,
Leung
PC,
Wong
ELY,
et
al.
Using
herbal
medicine
as
a
means
of
preven5on
experience
during
the
SARS
crisis.
Am.
J.
Chin.
Med.
2005;33(3):345-‐356.