1. Literature Synthesis
1.Citrate reactions are uncommon and
usually mild when they do occur.
2.Consider prophylactic calcium in
donors with low body weight, liver or
kidney dysfunction, or those with a
history of citrate reactions.
3.Intravenous calcium gluconate is
associated with extravasation necrosis
and multiple drug interactions.
Literature Synthesis
1.Citrate reactions are uncommon and
usually mild when they do occur.
2.Consider prophylactic calcium in
donors with low body weight, liver or
kidney dysfunction, or those with a
history of citrate reactions.
3.Intravenous calcium gluconate is
associated with extravasation necrosis
and multiple drug interactions.
Background
Citrate is an anticoagulant used during
apheresis procedures. It achieves
anticoagulation of the extracorporeal
apheresis circuit by temporarily binding to
free calcium in the blood causing symptoms
of hypocalcemia in some patients. Current
practice at our facility is to administer
prophylactic intravenous calcium gluconate
to every apheresis patient to prevent citrate
reactions. An additional dose is given for
any type of citrate reaction., regardless of
severity.
Problem
There have been national shortages of
intravenous calcium gluconate. This has led
to time-consuming efforts for the apheresis
nursing staff. Those efforts include
additional communication with the
physicians , re-scheduling lower priority
procedures, and coordinating with
pharmacy.
Project Description
This project was focused on the donor
population served at our facility. Donor
citrate reactions were managed based on
clinical assessment of symptoms rather
than prophylactically.
PICO Question
Are oral calcium carbonate supplements as
effective as intravenous calcium gluconate
in managing mild citrate reactions in
apheresis donors?
Background
Citrate is an anticoagulant used during
apheresis procedures. It achieves
anticoagulation of the extracorporeal
apheresis circuit by temporarily binding to
free calcium in the blood causing symptoms
of hypocalcemia in some patients. Current
practice at our facility is to administer
prophylactic intravenous calcium gluconate
to every apheresis patient to prevent citrate
reactions. An additional dose is given for
any type of citrate reaction., regardless of
severity.
Problem
There have been national shortages of
intravenous calcium gluconate. This has led
to time-consuming efforts for the apheresis
nursing staff. Those efforts include
additional communication with the
physicians , re-scheduling lower priority
procedures, and coordinating with
pharmacy.
Project Description
This project was focused on the donor
population served at our facility. Donor
citrate reactions were managed based on
clinical assessment of symptoms rather
than prophylactically.
PICO Question
Are oral calcium carbonate supplements as
effective as intravenous calcium gluconate
in managing mild citrate reactions in
apheresis donors?
Citrate Reactions
MILD
•Circumoral numbness and tingling
MODERATE
•Chills
•Vibration sensation
•Non-cardiac chest heaviness
•Nausea
SEVERE
•Tetany
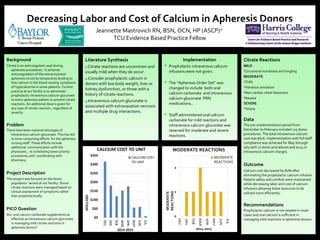
Data
The pre-implementation period from
December to February included 115 donor
procedures. The total intravenous calcium
cost was $616. Implementation with full staff
compliance was achieved for May through
July with 77 donor procedures and $124 in
intravenous calcium charges..
Outcome
Calcium cost decreased by 80% after
eliminating the prophylactic calcium infusion.
Patient safety and comfort were maintained
while decreasing labor and cost of calcium
infusions allowing these resources to be
utilized more efficiently.
Recommendations
Prophylactic calcium is not needed in most
cases and oral calcium is sufficient in
managing mild reactions in apheresis donors.
Citrate Reactions
MILD
•Circumoral numbness and tingling
MODERATE
•Chills
•Vibration sensation
•Non-cardiac chest heaviness
•Nausea
SEVERE
•Tetany
Data
The pre-implementation period from
December to February included 115 donor
procedures. The total intravenous calcium
cost was $616. Implementation with full staff
compliance was achieved for May through
July with 77 donor procedures and $124 in
intravenous calcium charges..
Outcome
Calcium cost decreased by 80% after
eliminating the prophylactic calcium infusion.
Patient safety and comfort were maintained
while decreasing labor and cost of calcium
infusions allowing these resources to be
utilized more efficiently.
Recommendations
Prophylactic calcium is not needed in most
cases and oral calcium is sufficient in
managing mild reactions in apheresis donors.
Implementation
Prophylactic intravenous calcium
infusions were not given.
The “Apheresis Order Set” was
changed to include both oral
calcium carbonate and intravenous
calcium gluconate PRN
medications..
Staff administered oral calcium
carbonate for mild reactions and
intravenous calcium gluconate was
reserved for moderate and severe
reactions.
Implementation
Prophylactic intravenous calcium
infusions were not given.
The “Apheresis Order Set” was
changed to include both oral
calcium carbonate and intravenous
calcium gluconate PRN
medications..
Staff administered oral calcium
carbonate for mild reactions and
intravenous calcium gluconate was
reserved for moderate and severe
reactions.
Decreasing Labor and Cost of Calcium in Apheresis Donors
Jeannette Mastrovich RN, BSN, OCN, HP (ASCP)cm
TCU Evidence Based Practice Fellow