Ndcr inc application for men and women website
•Download as DOCX, PDF•
0 likes•138 views


Recommended
More Related Content
Viewers also liked
Viewers also liked (10)
Similar to Ndcr inc application for men and women website
Similar to Ndcr inc application for men and women website (20)
Ndcr inc application for men and women website
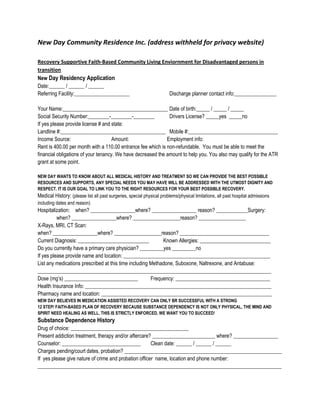
- 1. New Day Community Residence Inc. (address withheld for privacy website)<br />Recovery Supportive Faith-Based Community Living Enviornment for Disadvantaged persons in transition<br />New Day Residency Application<br />Date:______ / ______ / ______<br />Referring Facility:_____________________Discharge planner contact info:________________<br />Your Name:________________________________________Date of birth:_____ / _____ / _____<br />Social Security Number:________-________-________Drivers License? _____yes _____no<br />If yes please provide license # and state:<br />Landline #:________________________________________Mobile #:__________________________________<br />Income Source: Amount: Employment info: <br />Rent is 400.00 per month with a 110.00 entrance fee which is non-refundable. You must be able to meet the financial obligations of your tenancy. We have decreased the amount to help you. You also may qualify for the ATR grant at some point. <br />NEW DAY WANTS TO KNOW ABOUT ALL MEDICAL HISTORY AND TREATMENT SO WE CAN PROVIDE THE BEST POSSIBLE RESOURCES AND SUPPORTS, ANY SPECIAL NEEDS YOU MAY HAVE WILL BE ADDRESSED WITH THE UTMOST DIGNITY AND RESPECT. IT IS OUR GOAL TO LINK YOU TO THE RIGHT RESOURCES FOR YOUR BEST POSSIBLE RECOVERY.<br />Medical History: (please list all past surgeries, special physical problems/physical limitations, all past hospital admissions including dates and reason)<br />Hospitalization:when? _________________where? _________________ reason? ____________Surgery:when? _________________where? __________________reason? __________________<br />X-Rays, MRI, CT Scan:<br />when? _________________where? __________________reason? __________________________________<br />Current Diagnosis: ___________________________ Known Allergies: ___________________________<br />Do you currently have a primary care physician? _________yes _________no<br />If yes please provide name and location: ________________________________________________________<br />List any medications prescribed at this time including Methadone, Suboxone, Naltrexone, and Antabuse: _________________________________________________________________________________________<br />Dose (mg’s) ____________________________Frequency: ____________________________________<br />Health Insurance Info: _______________________________________________________________________<br />Pharmacy name and location: _________________________________________________________________<br />NEW DAY BELIEVES IN MEDICATION ASSISTED RECOVERY CAN ONLY BR SUCCESSFUL WITH A STRONG <br />12 STEP/ FAITH-BASED PLAN OF RECOVERY BECAUSE SUBSTANCE DEPENDENCY IS NOT ONLY PHYSICAL, THE MIND AND SPIRIT NEED HEALING AS WELL. THIS IS STRICTLY ENFORCED, WE WANT YOU TO SUCCEED!<br />Substance Dependence History<br />Drug of choice: _____________________________________________<br />Present addiction treatment, therapy and/or aftercare? ________________________ where? _________________<br />Counselor: ______________________________Clean date: ______ / ______ / ______<br />Charges pending/court dates, probation? ____________________________________________________________<br />If yes please give nature of crime and probation officer name, location and phone number: _____________________________________________________________________________________________<br />Emergency Contact Info / Next of Kin including phone info and address; <br />Relationship to you: ________________________________________<br />Release signed and witnessed by staff? <br />Please list 3 personal goals you would like to accomplish for recovery:<br />1:<br />2:<br />3:<br />Acts of violence, substance, medication misuse, non-payment of fees, rule-breaking or non-compliance will be grounds for dismissal. We will not tolerate violence, fighting, and/or drug or alcohol use. We are committed to helping you and will discuss with you any early warning signs of relapse behavior to prevent dismissal. Ultimately, you are responsible for your recovery. You can do this!<br />Staff Use Only:<br />Acceptance Date:<br />Residency Date:Anticipated Departure Date:<br />Exit Interview?<br />Exit description and reason:<br />Tox Screens:<br />Date:Result:Date:Result:Date:Result:<br />Date:Result:Date:Result:Date:Result:<br />