1. Building a Clinical Model for Improved Linkage and Navigation
within the HCV Cascade of Care
Alexander G. Geboy1, Hyun A. Cha1, Idene E. Perez1, Sean N. Patterson1, Matthew T. Bell1, Adebisi O. Ayodele2, Dawn A. Fishbein1,2
1MedStar Health Research Institute, 2MedStar Washington Hospital Center
80006
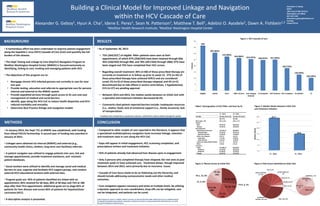
• As of September 30, 2015:
• 75% (264/353*) of eligible RNA+ patients were seen at their
appointment, of which 97% (258/264) have been retained through 60d,
95% (250/264) through 90d, and 78% (207/264) through 180d; 97% have
been staged and 73% have completed their HCC screen.
• Regarding overall treatment: 46% (n=60) of those prescribed therapy are
currently on treatment or in follow up prior to week 12; 27% (n=35) of
those prescribed therapy have achieved SVR12 and are considered
cured; 2% (n=3) of those prescribed therapy relapsed; and 4% (n=5)
discontinued due to side effects (1 severe renal failure, 1 hypokalemia);
21% (n=27) are pending approval.
• Between 2014 and 2015, the median weeks between an initial visit with
a specialist and treatment initiation decreased 50.3%.
• Commonly cited patient-reported barriers include: inadequate resources
(i.e., shelter, food), lack of emotional support (i.e., family structure), lack
of transportation.
* 12 patients were removed due to spontaneous clearance and therefore could not advance through the cascade
• Compared to other models of care reported in the literature, it appears that
a specialized multidisciplinary navigation team increases linkage, retention
and treatment rates in care along the HCV CoC.
• Gaps still appear in initial engagement, HCC screening completion, and
prescriptions written and treatment initiation.
• 42% of patients already had advanced liver disease upon re-engagement.
• Only 3 persons who completed therapy have relapsed; the rest seen at post
treatment week 12 have achieved cure. Treatment delays, though improved
between 2014 and 2015, were primarily due to insurance issues.
• Cascade of Care focus needs to be on flattening out the hierarchy, and
should include addressing socioeconomic needs and other medical
outcomes.
• Care navigation appears necessary and exists at multiple levels. By utilizing
a dynamic approach to care coordination, drop-offs can be mitigated, care
can be integrated, and patients can be cured.
RESULTSBACKGROUND
• A tremendous effort has been undertaken to improve patient engagement
along the hepatitis C virus (HCV) Cascade of Care (CoC) and quantify the full
burden of this disease.
• The HepC Testing and Linkage to Care (HepTLC) Navigation Program at
MedStar Washington Hospital Center (MWHC) is focused exclusively on
identifying, linking to care, treating and managing patients with HCV.
• The objectives of this program are to:
• Reengage chronic HCV-infected persons not currently in care for over
one year
• Provide testing, education and referrals to appropriate care for persons
internal and external to the MWHC system
• Provide expedited services through quick access to ID care and case
management of medical and social barriers
• Identify gaps along the HCV CoC to reduce health disparities and HCV-
induced morbidity and mortality
• Determine Best Practice linkage and navigation models
METHODS
• In January 2014, the HepC TLC at MWHC was established, with funding
from Gilead FOCUS Partnership. A second year of funding was awarded in
January of 2015.
• Linkages were obtained via internal (MWHC) and external (e.g.,
community health clinics, shelters, long-term care facilities) referrals.
• A patient navigator was utilized to engage patients into care, link and
manage appointments, provide treatment assistance, and maintain
patient databases.
• Social workers were utilized to identify and manage social and medical
barriers to care, organize and facilitate HCV support groups, and conduct
external HCV-educational sessions with external sites.
• Program goals are: 95% of patients identified are linked with an
appointment, 85% retained for 60 days, 80% at 90 days and 75% at 180
days after their first appointment. Additional goals are to stage 85% of
patients for liver disease and screen 85% of patients for hepatocellular
carcinoma (HCC).
• A descriptive analysis is presented.
CONCLUSION
Alexander G. Geboy
MHRI
100 Irving St NW, EB 4111
Washington, DC 20010
267-322-1228
Alexander.g.geboy@medstar.net
Funding:
Gilead FOCUS
365
307 (84%)
276 (90%)
264 (86%) 255 (97%) 248 (97%) 251 (95%)
182 (73%)
130 (49%)
103 (39%)
0
50
100
150
200
250
300
350
400
Eligible Linked Seen RNA+ & Seen Liver Staging
Ordered
LS Complete HCC Ordered HCC Complete Rx Written Tx
Patients
Figure 1: HCV Cascade of Care
0.0
5.0
10.0
15.0
20.0
25.0
30.0
Y1 - 2014 Y2 - 2015
27.7
13.8
MedianWeeks
F4, 64, 26%
F3-4, 3, 1%
F3, 36, 15%
F2, 35,
14%
F1-2, 50,
20%
F1, 9, 4%
F0-1, 15, 6%
F0, 36,
14%
IVDU, 166, 33%
INTRANASAL
COCAINE, 120, 24%
SEXUAL (HETERO),
53, 10%
JAIL, 46, 9%
BLOOD TRANS, 44,
9%
TATOO, 36, 7%
DENIED, 23, 5%
MSM, 6, 1%
OCC. HZ, 4,
1%
UNKNOWN, 4,
1%
PERINATAL, 2, 0%
Other, 16, 3%
Table1: Demographics of HCV RNA+ and Seen by ID Figure 2: Median Weeks between Initial Visit
and Treatment Initiation
Figure 3: Fibrosis Scores at Initial Visit Figure 4: Risk Factors Identified at Initial Visit
Author Disclosures: Dawn A. Fishbein, MD has served on an Advisory Board for BMS, Gilead and serves as a Medical Advisor
for Hepatitis Foundation International; Alexander G. Geboy has served on an Advisory Board for Gilead Sciences, LLC. Both
have grant funding from Gilead Sciences.
Y1 - 2014 Y2 - 2015
Variable Number (Percent) Number (Percent)
(N=177) (N=99)
Mean Age + SD 59.2 + 8.6 60.5 + 7.8
Gender
Men 99 (55.9) 60 (60.6)
Women 78 (44.1) 39 (39.4)
Race/Ethnicity
black/African American 165 (93.2) 88 (88.9)
black/AA Men 91 (55.2) 54 (61.4)
black/AA Women 74 (44.8) 34 (38.6)
white, non-Hispanic 9 (5.1) 4 (4.0)
white Men 7 (77.8) 2 (50.0)
white Women 2 (22.2) 2 (50.0)
American Indian/Alaska Native 2 ( 1.1) 2 (2.0)
Other 1 (0.6) 5 (5.1)
Insurance
Public 143 (80.8) 80 (80.8)
Medicare 52 (36.4) 28 (35.0)
Medicaid 91 (63.6) 52 (65.0)
Private 34 (19.2) 19 (19.2)