CALL ON ➥9907093804 🔝 Call Girls Baramati ( Pune) Girls Service
COPD
1. 1
Mental Health Consultation
Patient Name: COPD Facility: XXXX
Date: 4-9-13
Additional history can be found elsewhere in this chart and will not be repeated here.
Reasonfor Referral: xx-year-old, white, xxxx, female… I was asked to evaluate her for
depression.
Current Medications: Zoloft 150mg qhs, Prednisone, Diltiazem, Omeprazole, Cozaar,
Klonopin 0.5mg bid and 0.5mg tid prn, Cardizem
Medical History: Bronchiolitis obliterans, Depressive Disorder, Anxiety Disorder, Type II
Diabetes Mellitus, Hypertension, Carotid Artery Disease, Osteoarthritis, Hypertensive Heart
Disease; She is both steroid dependent and oxygen dependent.
Mental Status Exam: She was an alert, cooperative, extremely thin almost cachectic, anxious
and depressed looking woman. She complained of feeling depressed. She said her appetite was
improving and her sleep was okay. Her speech was slow but coherent and relevant. Her affect
was flat. Her thought content revolved mostly around complaints about her daughter whom she
characterized as “uncaring”… “She blames me for the depression …She left last time saying “I
can’t take this anymore”…that is why my son is my health care agent”. There were no overt
signs of psychosis or delirium. She exhibited some memory problems. She did not know the
date, the day of the week or the name of the nursing home. She thought she was continuously a
resident of XXXX since last November. She made an odd remark, attributing her current
depression to a single incident of sexual abuse when she was 8-years-old.
Findings and Recommendations:
There are several interacting problems here. First, she appears to have a mild dementia. Based on
risk factors and clinical presentation, it is probably a vascular dementia (VaD). The VaD makes
her vulnerable to delirium. Her history suggests recent episodes of mild delirium. She was
recently treated for pneumonia a possible cause of delirium. She does not appear to be delirious
now. She is oxygen dependent and I suspect that low O 2 sats have been affecting her cognition.
She does exhibit a number of signs of vascular dementia including: memory impairment, lack of
spontaneity, psychomotor slowing, fatigue, loss of vigor, general dilapidation in cognitive
functioning, apathy and fluctuating mental status.
Furthermore, she is clinically depressed and quite anxious. The precipitants for her depression
include the death of her husband, family conflict and her failing health. The anxiety is in part a
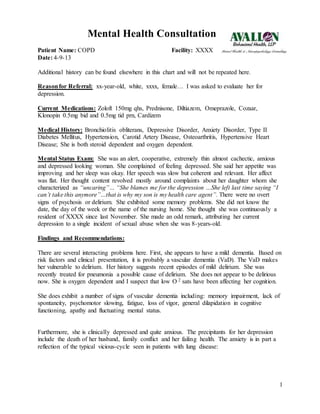
reflection of the typical vicious-cycle seen in patients with lung disease:
2. 2
1. I think we could provide her with more anxiety relief by changing her antidepressant
medication to one which has a greater anxiolytic effect. Therefore, would reduce Zoloft
to 75mg qd and start Lexapro 10mg qd x one week then reduce Zoloft to 50mg qd and
increase Lexapro to 20mg qd x one week then DC Zoloft and start Abilify 2mg qd
2. Need to be cautious in the use of benzodiazepines in patients with lung disease because
they suppress respiration especially during sleep. Therefore, would not give any
Klonopin dose after 4 PM.
3. Teach her to disrupt the above vicious-cycle through the use of visualization and
relaxation techniques
4. Encourage her to verbally vent her feelings of loss related to her husband’s death and her
declining health and her anger towards family members.
5. Obtain any neuroimaging which may have been done in the past. If unavailable, a brain
MRI would be helpful.
___________________________
Drew Chenelly, Psy.D.
Clinical Neuropsychologist
respiratorty
distress leads to
anxiety
anxiety leads to
hyperaroused
autonomic nervous
system with rapid
shallow, breathing
feelings of
suffocation
with associated fear
fear increases anxiety and
it’s attendant physical
sensations, which in turn
increases fear and anxiety
and so on
attentive to
breathing and fear
off suffocation