Recommended

Recommended
More Related Content
What's hot
What's hot (19)
Similar to Ozioma Njoku
Similar to Ozioma Njoku (20)
Recently uploaded
Recently uploaded (20)
Ozioma Njoku
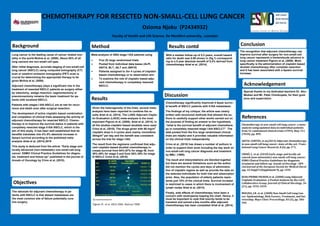
- 1. CHEMOTHERAPY FOR RESECTED NON-SMALL-CELL LUNG CANCER Ozioma Njoku (P2434932) Faculty of Health and Life Science. De Montfort university , Leicester Background Objectives Method Discussion Results Conclusion Acknowledgement References Lung cancer is the leading cause of cancer related mor- tality in the world Molina et al, (2008). About 85% of all lung cancers are non-small cell type. After initial diagnosis, accurate staging of non-small-cell lung cancer (NSCLC) using computed tomography (CT) scan or positron emission tomography (PET) scan is crucial for determining the appropriate therapy to be given Molina et al, (2008). Adjuvant chemotherapy plays a significant role in the treatment of resected NSCLC patients as surgery either by lobectomy, wedge resection, segmentectomy or pneumonectomy remains the basic treatment for pa- tients with localized NSCLC. Patients with stages I-IIIA NSCLC are at risk for recur- rence and death even after surgical resection. The development of active cisplatin based combination and completion of clinical trials assessing the activity of adjuvant chemotherapy for resected NSCLC. Chemo- therapy is to improve the survival status in patients with completely resected stage II-IIIA NSCLC, which is the aim of this study. It has been well established that its benefits translates into 4%-5% absolute increase in 5years survival according to the published meta- analysis Artal et al, (2014).2010 This study is deduced from the article ‘’Early stage and locally advanced (non-metastatic) non-small-cell-lung cancer: ESMO Clinical Practice Guidelines for diagno- sis, treatment and follow-up’’ published in the journal of Annals of Oncology by Crino et al, (2010). Meta-analysis of 4584 stage I-IIIA patients using Five (5) large randomised trials Pooled from individual data bases (ALPI, ANITA, BLT, IALT and JBR10) Patients assigned to 3or 4 cycles of cisplatin based chemotherapy or to observation arm To examine the role of cisplatin based adju- vant chemotherapy in completely resected NSCLC. Chemotherapy significantly improved 4-5year surviv- al benefit of NSCLC patients with II-IIIA metastases. The findings of my critique; the article was clearly written with structured methods that allowed the au- thors to carefully support other works carried out on the purpose of finding an answer to the hypothesis ‘’what is the survival benefit of adjuvant chemothera- py in completely resected stage I-IIIA NSCLC?’’. The data pooled from the five large randomised clinical trials are helpful and it provides valuable information on the clinical trials independently. Crino et al, (2010) has drawn a number of authors in order to support their work including the key work on non-small-cell lung cancer diagnosis and treatment by BMJ. (1995). The result and interpretations are blended together but there are several limitations such as the author did not mention the cycles and days of administra- tion of cisplatin regime as well as provide the data on the selected individuals for both trial and observation arms. Also, the population of elderly patients repre- sents just 10% of the clinical trials. Survival increase is restricted to cases in which there is involvement of lymph nodes Artal et al, (2014). Finally, side effects of chemotherapy have been a concern with neutropenia topping the chart. Hence, it must be important to note that toxicity tends to be transient and solved a few months after adjuvant chemotherapy has been completed Artal et al, (2014). Special thanks to my dedicated teachers Dr. Abu- Median and Mr. Peter Chimkupete, for their guid- ance and supervision. Chemotherapy in non-small cell lung cancer: a meta- analysis using updated data on individual patients from 52 randomised clinical trials (1995). Bmj, 311 (7010), pp. 899. ARTAL CORTÉS, et al,(2015) Adjuvant chemotherapy in non-small cell lung cancer: state-of-the-art. Trans- lational Lung Cancer Research, 8 (2), pp. 595. CRINÒ, L. et al. (2010) Early stage and locally ad- vanced (non-metastatic) non-small-cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology : Offi- cial Journal of the European Society for Medical Oncol- ogy, 25 Suppl 9 (Supplement 9), pp. v559. JEAN-PIERRE PIGNON et al. (2008) Lung Adjuvant Cisplatin Evaluation: A Pooled Analysis by the LACE Collaborative Group. Journal of Clinical Oncology, 22 (21), pp. 3552-3559. MOLINA, J.R. et al. (2008) Non-Small Cell Lung Can- cer: Epidemiology, Risk Factors, Treatment, and Sur- vivorship. Mayo Clinic Proceedings, 83 (5), pp. 584- 594. The recognition that adjuvant chemotherapy can improve survival after surgery for non-small-cell lung cancer represents a tremendouds advance in lung cancer treatment Pignon et al, (2008). More specifically is the administration of cisplatin based doublet chemotherapy after complete resection and it has been associated with a 5years survival increase. Given the heterogeneity of the trials, several meta- analysis have been reported to combine the re- sults Artal et al, (2014). The LUNG Adjuvant Cispla- tin Evaluation (LACE) meta-analysis is the most important Pignon et al, (2008); Artal et al, (2014). In all the studies cisplatin-based doublets were used Crino et al, (2010). The drugs given with 80 mg/m2 cisplatin dose in 4 cycles were mainly vinorelbine 30mg/m2 per day and the benefit was consistent across the trial for stage I-IIIA. The result from the regimens confirmed that adju- vant cisplatin-based doublet chemotherapy in- crease survival from 64%-67% for stage IB, from 39%-49% for stage II and from 26%-39% for stage III NSCLC Crino et al, (2010). The rationale for adjuvant chemotherapy in pa- tients with NSCLC is that distant metastases are the most common site of failure potentially cura- tive surgery. With a median follow-up of 5.2 years, overall hazard ratio for death was 0.89 shown in (fig.1) correspond- ing to a 5 year absolute benefit of 5.4% derived from chemotherapy Artal et al, (2014). Results contd Fig.1 overall survival by trial Pignon JP, et al. ASCO 2006. Abstract 7008