
Recommended
More Related Content
Similar to Xray findings- MM,TB.ID.pptx
Similar to Xray findings- MM,TB.ID.pptx (20)
More from CharitheLakshitheCha
Recently uploaded
Recently uploaded (20)
Xray findings- MM,TB.ID.pptx
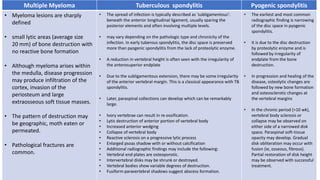
- 1. Multiple Myeloma Tuberculous spondylitis Pyogenic spondylitis • Myeloma lesions are sharply defined • small lytic areas (average size 20 mm) of bone destruction with no reactive bone formation • Although myeloma arises within the medulla, disease progression may produce infiltration of the cortex, invasion of the periosteum and large extraosseous soft tissue masses. • The pattern of destruction may be geographic, moth eaten or permeated. • Pathological fractures are common. • The spread of infection is typically described as 'subligamentous': beneath the anterior longitudinal ligament, usually sparing the posterior elements and often involving multiple levels. • may vary depending on the pathologic type and chronicity of the infection. In early tuberous spondylitis, the disc space is preserved more than pyogenic spondylitis from the lack of proteolytic enzyme. • A reduction in vertebral height is often seen with the irregularity of the anterosuperior endplate • Due to the subligamentous extension, there may be some irregularity of the anterior vertebral margin. This is a classical appearance with TB spondylitis. • Later, paraspinal collections can develop which can be remarkably large. • Ivory vertebrae can result in re-ossification. • Lytic destruction of anterior portion of vertebral body • Increased anterior wedging • Collapse of vertebral body • Reactive sclerosis on a progressive lytic process • Enlarged psoas shadow with or without calcification • Additional radiographic findings may include the following: • Vertebral end plates are osteoporotic. • Intervertebral disks may be shrunk or destroyed. • Vertebral bodies show variable degrees of destruction. • Fusiform paravertebral shadows suggest abscess formation. • The earliest and most common radiographic finding is narrowing of the disc space in pyogenic spondylitis. • It is due to the disc destruction by proteolytic enzyme and is followed by irregularity of endplate from the bone destruction. • In progression and healing of the disease, osteolytic changes are followed by new bone formation and osteosclerotic changes at the vertebral margins • In the chronic period (>10 wk), vertebral body sclerosis or collapse may be observed on either side of a narrowed disk space. Paraspinal soft-tissue opacity may develop. Gradual disk obliteration may occur with fusion (ie, osseous, fibrous). Partial restoration of disk height may be observed with successful treatment.
- 2. MRI findings of pyogenic and tuberculous spondylitis
- 3. Multiple Myeoloma - Xray