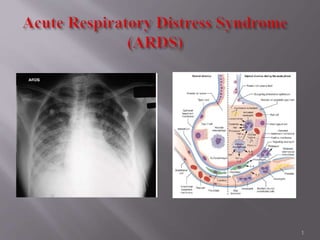
2. a clinical syndrome of severe dyspnea of rapid
onset, hypoxemia, and diffuse pulmonary infiltrates
leading to respiratory failure.
caused by diffuse lung injury from many underlying
medical and surgical disorders.
23. Bedside flexible fiberoptic bronchoscope with BAL
Protein (lavage/serum) <0.5 = Hydrostatic edema
Protein (lavage/serum) >0.7 = Lung inflammation
BAL cells 80% NeutrophilsARDS
23
24. Sensitive than CXR
Earlier detection.
Patchy abnormalities with increased density in dependent
lung zones.
Also detects pneumothorax, effusions and
pneumomediastinum, cavitation, and mediastinal
lymphadenopathy.
Potential benefit must be weighed against the risk
associated with transporting a critically ill patient.
24
25. Echocardiography.
(Brain Natriuretic Peptide) BNP <100 pg/ml suggestive
of ARDS/ALI.
Invasive Hemodynamic Monitoring
A PCWP<18 mm Hg consistent with noncardiogenic
Supporting evidence of Sepsis
Fluid Management
25
26. Treatment of the underlying disorders
Mechanical Ventilation
Prophylaxis against
DVT
Stress Ulcer
Aspiration
CVP infections
Prompt recognition of nosocomial infections
Adequate nutrition.
26
27. Sometimes CPAP ventilation alone may be
sufficient to improve oxygenation.
Less invasive, less complication.
Lack of enough study and lack of definite
guidelines.
27
28. Goals
Maintain oxygenation.
Avoid oxygen toxicity.
Avoid complications of mechanical ventilation.
Target
SpO2 @ 85-90% with FIO2< 65% within first 24-48
hours.
28
29.
30.
31. Conventional tidal volume12 mL/kg
Low tidal volume6ml/kg
was associated with a 9% (absolute) reduction in
mortality when the end inspiratory plateau pressure
was <30 cm H2O (18).
31
33. One of the consequences of low volume ventilation is
hypercapnia and respiratory acidosis.
Data from clinical trials shows PCO2 60 -70 mm Hg
with pH-7.2- 7.25 safe for most patients.
Brainstem respiratory stimulation with subsequent
hyperventilationventilator asynchrony.
Hypercapneic acidosis may down-regulate
inflammatory cell activity, and may inhibit xanthine
oxidase, thus reducing oxidant stress. 33
34. 1. PEEP
Collapse of terminal airways at
the end of expiration.
PEEP act as a stent to keep
small airways open at the end
of expiration.
Allows a reduction in theFiO2
to safer levels.
Reduction of Cardiac Output.
34
36. 2.“Inverse Ratio ventilation”
Increasing Inspiration time such that I:E > 1:1
Advantage of improving oxygenation allowing FI02
reduction.
Diminished time to exhale, dynamic hyperinflation leading
to increased end-expiratory pressure, similar to ventilator
prescribed PEEP(Auto-PEEP generation)
Sedation & Paralysis.
No mortality benefit in ARDS has been demonstrated.
36
37. Partial liquid ventilation (PLV) with perfluorocarbon
An inert, high-density liquid that easily solubilizes oxygen
and carbon dioxide
Filling the lung with liquid removes the air-liquid interface
and supports alveoli thus preventing their collapse
Promising preliminary tests
Associated with increased incidence of pneumothorax,
mucus plugging and disruption of normal surfactant system
Lung-replacement therapy with extracorporeal membrane
oxygenation (ECMO) - survival benefit in neonatal
respiratory distress syndrome, may also have utility in select
adult patients with ARDS.
37
38. Maintain a normal or low left atrial filling pressure
Minimizes pulmonary edema
prevents further decrements
in arterial oxygenation
lung compliance
Shortens
ICU stay
duration of mechanical ventilation
limited by
Hypotension -- Add up to reduce venous return by PEEP
“Diuretics don't reduce inflammation’’ 38
43. A randomized, clinical trial determined that
simvastatin, a hydroxymethylglutaryl-coenzyme A
reductase inhibitor,improved oxygenation and
respiratory mechanics in patients with ALI. Further
studies are needed, but treatment with simvastatin
appears safe and may be associated with improved
organ dysfunction in patients with ALI.
43
47. Rationale for Use
BAL from patients with ARDS have lower concentrations
of surfactant proteins.
Successful trials in premature infants.
Improve oxygenation acutely.
Rapid weaning from mechanical ventilation.
47
48. Basis for Recommendation
More recruitment of atelectatic dorsal lung regions
Decrease in abdominal compression of the thorax
Mobilisation and removal of secretions
Improve oxygenation in 70% of patients with ARDS
Effect that persists in 50% after returning to the supine
position.
Repositioning critically ill patients can be
hazardous
48
58. Begin within 48-72 hours of mechanical ventilation.
Tube feeding preferable to IV hyperalimentation.
A low-carbohydrate high-fat formula.
Include anti-inflammatory and vasodilating components
with antioxidants as supported by few studies.
58
59.
60.
61. Recent mortality estimates for ARDS range from 26 to 44%.
Mortality in ARDS is largely attributable to nonpulmonary
causes, with sepsis and nonpulmonary organ failure accounting
for >80% of deaths.
Advanced age ,Preexisting organ dysfunction are separate
predicotors of mortality.
Little value in predicting mortality from lung severity index
the PaO2/FIO2 ratio
the level of PEEP used in mechanical ventilation,
the respiratorycompliance,
the extent of alveolar infiltrates on chest radiography,
the lung injury score
61
62. Patients usually recover their maximum lung function
within 6 months.
One year after endotracheal extubation, more than one-
third of ARDS survivors have normal spirometry values
and diffusion capacity.
Severity Index & duration of mechanical ventilation are
associated with worse recovery of pulmonary function.
Significant rates of depression and PTSD in ARDS 62
Editor's Notes
Rough concept of chronological events
(after discussion of the main diagram) proliferative phase is a junction from where either resolution or fibrosis occurs. The presence of alveolar type III procollagen peptide, a marker of pulmonary fibrosis, is
associated with a protracted clinical course and increased mortality from ARDS
More characteristically there is predominant interstial odema and shift from neutrophil predominant to lymphocyte predominant infiltrate
Left hand show nice aerated alveolus with….
Under the influence of proinflammatory cytokines released by macrophages, neutrophils initially undergo sequestration in the pulmonary microvasculature, followed by margination and egress into the alveolar space.
organization of alveolar exudates forming hyaline membrane
The neutrophils then release the contents of their cytoplasmic
granules (i.e., proteolytic enzymes and toxic oxygen metabolites), and this
damages the endothelium and leads to a
leaky-capillary type of exudation into the lung parenchyma
As a part of reparative process or resoultion,
Resorption of alveolar edema fluid ….surfactant…..differentiate into type one
While many patients with ARDS recover lung function 3–4 weeks after the initial pulmonary injury, some will enter a
fibrotic phase that may require long-term support on mechanical ventilators and/or supplemental oxygen.
Histologically, the alveolar edema and inflammatory exudates of earlier phases are now converted to extensive
alveolar duct and interstitial fibrosis. Acinar architecture is markedly disrupted, leading to emphysema-like changes
with large bullae. Intimal fibroproliferation in the pulmonary microcirculation leads to progressive vascular occlusion
and pulmonary hypertension The physiologic consequences include an increased risk of pneumothorax, reductions
in lung compliance, and increased pulmonary dead space. Gradual remodeling and resolution of intraalveolar and interstitial granulation tissue and fibrosis are shown.
Putting this slide ahead For concept of lungs in Normal Spacious, roomy aerated alveoulos
Note the dense infiltration of inflammatory flooded with tiny dot like inflammatory
cells in ARDS and the obliteration of the distal airspaces.
In normal subjects, neutrophils make up less than 5% of the cells recovered
in lung lavage fluid, whereas in patients with ARDS, as many as 80% of the
recovered cells are neutrophils
eosinophilic pneumonia.
Pneumocystis.
the based upon
thermodilution cardiac output, right atrial pressure, and mean arterial pressure may provide
efficient. More
than 60% ARDS patients experience a (nosocomial) pulmonary infection either before or after the
onset of lung injury.
Because infection is often the underlying cause of ARDS, early administration of appropriate antibiotic therapy broad
enough to cover suspected pathogens is essential
Other important interventions in sepsis have included early goal-directed therapy, use of drotrecogin alfa (Xigris) in
selected patients with severe sepsis (APACHE score ≥25) and no contraindications, prevention of bleeding
complications by means of prophylaxis for deep venous thrombosis (DVT) and stress ulcers, early mobilization,
turning and skin care, removal of catheters and tubes as soon as possible, and elevation of the head of the bed and
other strategies to prevent ventilator-associated pneumonia, including facilitation of weaning from mechanical
ventilation by daily interruption of sedation coordinated with daily spontaneous breathing trials.
Because intubation and mechanical ventilation may be associated with an increased incidence of complications,
such as barotrauma and nosocomial pneumonia
Low tidal volumes (Vt)
may cause hypercapnia and atelectasis[1] due to their inherent tendency to increase Dead space
(physiology.
most substantial benefit in ARDS mortality
demonstrated for any therapeutic intervention in ARDS to date.
Marked reduction of lung compliance
absorption atelectasis, lung toxicity and possibly, systemic toxicity
set PEEP to minimize FIO2 and
optimize PaO2
air spaces that are filled with exudate and not recruitable, and (c) areas that are collapsed due to interstitial infiltration and are potentially recruitable. Recruitment is a strategy aimed at re-expanding collapsed lung tissue, and then maintaining high PEEP to prevent subsequent ‘de-recruitment
ARDS causes redistribution of pulmonary blood flow away from dependent lung regions that exhibit increased pulmonary vascular resistance (PVR) because of pulmonary edema. PEEP may lower the PVR hence improving V/Q matching by shifting pulmonary blood flow from non-dependant lung regions to dependant
The PEEP is effective in early ARDS, because it acts as a counterforce, preventing the compression atelectasis secondary to severe pulmonary edema whereas the fibro-proliferative processes may explain the lack of effects of PEEP in the late stage of ARDS
Through stepwise increases in PEEP (increments of 2-3), a level should be sought that maintains approximately 90% arterial oxygen saturation at 50-60% FiO2.
Application of PEEP beyond 15-20 cm H2O may result in decreased venous return (hence ensure normal volume prior to starting PEEP), in turn reducing the cardiac output If volume loading is insufficient, the next step to restore cardiac output would be to add inotropes. If cardiac output still remains depressed, PEEP needs to be decreased stepwise until cardiac output is restored
PEEP optimization may lead to lung protection via mechanisms other than alveolar recruitment -for example, by avoiding surfactant depletion and disruption occurring at low end-expiratory lung volumes.24
There are normal
alveoli which are always inflated and engaging in gas exchange, flooded alveoli which can never,
under any ventilatory regime, be used for gas exchange, and atelectatic or partially flooded alveoli
that can be "recruited" to participate in gas exchange under certain ventilatory regimens. The
recruitable aveoli represent a continuous population, some of which can be recruited with minimal
PEEP, and others which can only be recruited with high levels of PEEP. An additional complication is
that some or perhaps most alveoli can only be opened with higher airway pressures than are needed
to keep them open
the use of CPAP or PEEP usually promotes improved oxygenation, allowing the FIO2 to be tapered.
With PEEP, positive pressure is maintained throughout expiration, but when the patient inhales spontaneously,
airway pressure decreases to below zero to trigger airflow. With CPAP, a low-resistance demand valve is used to
allow positive pressure to be maintained continuously.
In the ARDS Network clinical trial, it was concluded that in patients with acute lung injury and ARDS who received mechanical ventilation with lower tidal volumes and inspiratory pressures (all patients received a tidalvolume goal of 6 ml per kilogram of predicted body weight and an inspiratory plateau pressure of 30 cm of water or less), raising PEEP to levels that exceeded those used in their lower-PEEP strategy (8.3±3.2 cm of water in the lower-PEEP group and 13.2±3.5 cm of water in the higher-PEEP group) did not achieve statistically significant survival benefit.27
On the other hand, there is the potential of developing dynamic hyperinflation and auto-PEEP (which may be undesirable) during inverse ratio ventilation (IRV), which is an extreme form of lengthening the Ti.
NEJM 1995 Review Article: ARDS & I:E
Inverse ratio ventilation should still be considered experimental since it has not been prospectively evaluated... therefore, until further studies
have been performed, we recommend that ‘reversal' be considered only when acceptable arterial oxygenation cannot be achieved with a PEEP
<15 cm H20 or when the use of PEEP is associated with excessive peak airway pressures.
However, “Reverse Ventilation” usually requires heavy sedation & paralysis
hypoperfusion of critical organs
Diuretic therapy can then be tailored to achieve the lowest
cardiac filling pressures that do not compromise cardiac output and systemic
oxygen transport
They concluded that, if administered before end-stage fibrosis develops, methylprednisolone therapy could be effective in improving lung function and outcome in patients with unresolving ARDS
They concluded that, if administered before end-stage fibrosis develops, methylprednisolone therapy could be effective in improving lung function and outcome in patients with unresolving ARDS
increased risk of superinfections
Craig TR, Duffy MJ, Shyamsundar M, McDowell C, O'Kane CM, Elborn JS, et al. A Randomized Clinical
Trial of Hydroxymethylglutaryl- Coenzyme A Reductase Inhibition for Acute Lung Injury (The HARP Study) Am J Respir Crit Care Med. Mar 12011;183(5):620-6. [Medline].
Methemoglobinemia, decreased platelet aggregation and rebound deterioration in arterial oxygenation and elevation of pulmonary arterial pressure are significant possible side effects
Sildenafil
of phosphatidyl choline, phosphatidyl glycerol, and
Preferential deposition in healthy lung units, inactivation in damaged alveoli, and variable delivery systems may all contribute to failure in these trials.65
Leading to accidental endotracheal
extubation, loss of central venous catheters, and orthopedic injury
open lung approach
optimal level
of PEEP is just above the lower inflection point.
Using this approach, the average PEEP level required is 15.
unless it is contraindicated because of an acute abdomen,
ileus, GI bleeding, or other conditions.
eicosapentaenoic acid and linoleic acid
Risk factors predictive of increased mortality in ARDS/ ALI as reviewed by Vasudevan A et al include liver dysfunction, age, sepsis, HIV infection, oxygenation index, length of mechanical ventilation prior to ARDS, mechanism of lung injury, right ventricular dysfunction and PaO2/FiO2 ratio less than 100.
11,12,13,14 ,15 liver disease, cirrhosis, chronic alcohol abuse, chronic immunosuppression, sepsis chronic renal disease, any nonpulmonary organ failure, and increased APACHE III scores