Top Rated Bangalore Call Girls Ramamurthy Nagar ⟟ 9332606886 ⟟ Call Me For G...
BDSRA 2015 CLN6 Mole
1. Access to UCL e-resources
UCL Library Services, Gower St., London WC1E 6BT
020 7679 7700
E-mail: library@ucl.ac.uk
http://www.ucl.ac.uk/Library/
lease note
om 1 August 2009, UCL will no longer be using the Athens login for access to electronic
sources. You may still see links labelled "Athens login" on various resources, but these will
longer work for UCL members. The new access route for UCL users is outlined in this guide.
ccessing electronic resources via the UCL Library Services website
CL users are advised to access resources through the lists of ejournals
ttp://www.ucl.ac.uk/Library/ejournal) and databases (http://www.ucl.ac.uk/Library/database)
ailable on MetaLib. This will guarantee that you get free access to all the resources to which
u are entitled as a UCL member. If you are on-site you will not need to log in to resources. If
u are off-site, you will be prompted for your UCL userid and password automatically. This
echanism uses a so-called “proxy server” which simulates on-site access once you have
tered your UCL login.
ow do I log in to UCL e-resources?
any electronic resources do not require a login from computers on the UCL network. However,
you are using a computer which is not on the UCL network, then when you follow links to
Mole & Ali laboratory:
Variant Late Infantile Batten Disease
Sophia kleine Holthaus1,2, Sara Mole1, Sander Smith2, Robin Ali2
s.kleine.holthaus.11@ucl.ac.uk
1MRC Laboratory of Molecular Cell Biology
Gower Street, London WC1E 6BT
United Kingdom
Dr. Sara Mole
2Institute of Ophthalmology
11-43 Bath Street, London EC1V 9EL
United Kingdom
Prof. Robin Ali
• Loss of vision is one of the first symptoms in (juvenile) Batten disease and is characterised by loss of photoreceptors in
the retina. It precedes severe neurological symptoms and reduces quality of life of patients and affected families
signifcantly.
• Most of the therapies that are currently under investigation for Batten disease target the brain. It is unlikely that these
therapies have a beneficial effect on the eye.
• A treatment for the eye may delay the onset of the visual decline or slow down the progression of the vision loss. In the
future, a treatment for the eye and the brain could be combined.
• In comparison to the brain the eye is less complex, smaller and easy to access, which facilitates the delivery of therapeutic
components.
• For more information on gene therapy for the eye and the structure of the eye and retina please see concept poster “Gene
therapy for the eye”.
What is the purpose of a gene therapy for the eye?
What mouse model is good to test a therapy for the eye?
• Loss of vision is a key symptom in juvenile Batten disease. However, all mouse models that represent juvenile Batten
disease show only a mild visual decline and a slow degeneration of the retina making it difficult to test therapies in the eye.
• The Cln6 mouse, a model that represents a variant form of late infantile Batten disease, is a much better model because it
shows an early onset and faster progression of the retinal degeneration. In addition, the Cln6 mouse is deficient in a
transmembrane protein which poses very similar challenges for the development of a gene therapy as the mouse models of
juvenile Batten disease.
Aim of project
The aim of this project is to investigate how feasible a gene therapy is to improve vision in Batten disease. The ultimate goal
of this study is to improve quality of life of patients.
Step 1: Characterisation of vision loss in untreated Cln6 mice
Test for photoreceptor function
3w 1M 2M 3M 4M 5M 6M
Healthy
Mutant
Age
Healthy retina Mutant retina
Photo-
receptors
Photo-
receptors
Step 2: Delivery of viral vector carrying healthy Cln6
CLN6 virus
AAV8.CLN6 virus, high dose
Step 3: AAV8.CLN6 viral treatment of photoreceptors in Cln6 mice
Healthy
Mutant
Mutant, very high dose
Mutant, high dose
Mutant, moderate dose
Mutant, low dose
Test for photoreceptor function in treated mutant mice
1 month 2 months 4 months 6 months
CLN6 virus
Mutant, high dose Mutant, moderate dose Mutant, low doseHealthy retina
Photo-
receptors
Photo-
receptors
Step 4: Looking for a new target
It is important to understand when Cln6 mice start to loss vision and how it progresses over time. We found that:
• Photoreceptor function is progressively reduced from 3 weeks of age in
Cln6 mice (mutant) compared to healthy animals (A).
• Predominately photoreceptors are dying in the retina of mutant animals,
whereas the other two layers of the retina appear preserved (B).
A
B
The characterisation of the mutant Cln6 mice shows that
the function of photoreceptors is reduced and that
photoreceptors are dying.
Subretinal injections are ideal to deliver a virus to
photoreceptors throughout the retina. The cartoon depicts
the procedure in a human eye (A).
We performed subretinal injections of a virus carrying Cln6
(AAV8.Cln6) and show that the majority of photoreceptors
are targeted in the retina of a healthy mouse eye (B).
A B
Step 5: New virus targeting inner retina
Next, we injected mutant CLN6 mice subretinally with the AAV8.CLN6 virus and tested photoreceptor function. We found that:
• A very high dose of the virus
causes severe loss of photoreceptor
function indicating too much virus is
detrimental.
• Lower doses do not seem to
improve photoreceptor function as
the treated mutant eyes show a
p r o g r e s s i v e r e d u c t i o n o f
photoreceptor function similar to
untreated mutant eyes.
We investigated the structure of the retina to find out whether the viral treatment slowed down the photoreceptor loss. We found:
• The injection of the virus
introduced the expression of Cln6
in photoreceptors across all doses.
• However, none of the viral doses
p r e v e n t e d t h e l o s s o f
photoreceptors in the mutant mice.
CLN6
bipolar
Photo-
receptors
Inner retina,
e.g. bipolar
cells
Healthy retina
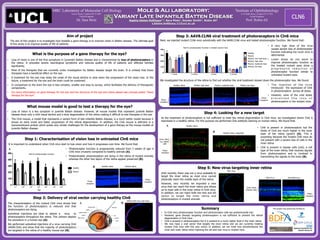
As the treatment of photoreceptors is not sufficient to treat the retinal degeneration in Cln6 mice, we investigated where Cln6 is
expressed in a healthy retina. For this purpose we performed Cln6 antibody staining on human retina. We found that:
• Cln6 is present in photoreceptors but the
levels of Cln6 are much higher in the inner
layer of the retina (green) (A). This is
surprising because the mutant Cln6 mice do
not present with a severe loss of cells in the
inner retina.
• Cln6 is present in bipolar cells (red), a cell
type of the inner retina, that receives signals
from photoreceptors and is involved in
transmitting the signals to the brain (B).
Healthy retina, magnified
B
A
New virus
Green virus
Photo-
receptors
New virus
Inner retina
(bipolar cells)
Old AAV8 virus
Until recently, there was not a virus available to
target the inner retina as most virus cannot
physically reach the middle layer of the retina.
However, very recently we imported a new
virus that can reach the inner retina and allows
us to treat cells in the inner retina in Cln6 mice.
In addition, we can inject both the new and old
vector to target the inner retina and
photoreceptors in mutant animals.
Summary
• In Cln6 mice photoreceptor function and photoreceptor cells are predominantly lost.
• However, gene therapy targeting photoreceptors is not sufficient to prevent the retinal
degeneration in Cln6 mice.
• Cln6 is present in photoreceptors but it is present to a much higher level in the inner retina.
• We now have a viral vector that targets the inner retina and we are currently treating
mutant Cln6 mice with this new vector. In addition, we can treat now simultaneously the
inner and outer retina when injecting the old and new virus in mutant mice.
Old AAV8 virus
This project was generously funded by: