Running Head MEDICARE POLICY Of 2019 MEDICARE POLIC.docx
MEXICO POSTER HEALTH ECONOMICS
1. Passed in 2003, the Sistema de Protección Social en Salud or System of Social
Protection in Health for the initiated the beginning of universal healthcare
coverage in Mexico
This would cover the poor who previously could not afford or qualify for
traditional Social Security the ability to apply for the Seguro Popular or
People’s Insurance
The Seguro Popular aims to achieve universal healthcare coverage for all
Mexican citizens by the year 2010
All access to care would be provided by the Ministry of Health and the
Instituto Mexicano de Seguridad Social
Public health services in Mexico are covered through the Ministry of Health as
well as the Fondo de Protección contra Gastos Catastróficos or Fund for
Protection against Catastrophic Expenditures (FPGC).
Other public health insurance payers come through those who are:
Self-employed
Out of the labor market
With the informal sector of the economy
Bonilla-Chacín, M. E., & Aguilera, N. (2013). The Mexican social protection system in health.
Gutiérrez, N. C. (2014, July). Mexico: availability and cost of health care – legal aspects.
Retrieved from https://www.justice.gov/sites/default/files/eoir/legacy/2014/07/14/2014-
010632%20MX%20RPT%20FINAL.pdf
Frenk, J., Gómez-Dantés, O., & Knaul, F. M. (2009). The democratization of health in Mexico:
financial innovations for universal coverage. Bulletin of the World Health Organization, 87,
542-548. doi:10.2471/BLT.08.053199
Organisation for Economic Co-Operation and Development. (2005). OECD reviews of health
systems: Mexico. Retrieved from http://www.borderhealth.org/files/res_839.pdf
Puig, A., Pagán, J. A., & Wong, R. (2009). Assessing quality across health care subsystems in
Mexico. Journal of Ambulatory Care Management, 32(2), 123-131.
doi:10.1097/JAC.0b013e31819942e5
World Health Organization. (2006, April). WHO country cooperation strategy at a glance.
Retrieved from
http://www.who.int/countryfocus/cooperation_strategy/ccsbrief_mex_en.pdf?ua=1
World Health Organization. (2015). Global Health Observatory. Mexico; Country Data and
Statics. Retrieved from http://www.who.int/gho/countries/mex.pdf?ua=1. March 24, 2015.
Unequal access, financing, and health outcomes as a result of segmentation in the
delivery of services
Need to guarantee high quality services and adequate health financing.
The need for additional public funding in order to extend access to care for non-
communicable diseases such as cardiovascular disease, diabetes, and cancer.
Healthcare disparities remain between the different states in Mexico due to socio-
economic factors:
Richer states benefit from more social insurance and resources for the
uninsured
Yet the rural populations remain underserved
Improving the fragmented insurance program as well as consolidating the Mexican
insurance system.
More attention in the area of healthcare quality:
More emphasis on preventive care
Increasing regulations on medical schools and certification of healthcare providers
OVERVIEW
FINANCING/ REIMBURSEMENT
PAYER SYSTEM
CHALLENGES
HEALTHCARE PROVIDERS
REFERENCES
WHO RANKING
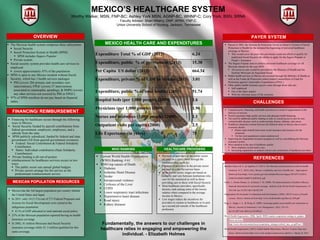
MEXICO HEALTH CARE AND EXPENDITURES
Fundamentally, the answers to our challenges in
healthcare relies in engaging and empowering the
individual. - Elizabeth Holmes
The Mexican health system comprises three subsystems:
Social Security
Social Protection System in Health (SPSS)
SPSS includes Seguro Popular
Private system.
Social security system provides health care services to
employed
covers approximately 47% of the population
SPSS is open to any Mexico resident without Social
Security, which has 3 health services packages
PHI (covers 284 primary and secondary care
interventions), FPGC (covers 57 interventions
associated to catastrophic spending), & SMPG (covers
any other services not covered by PHI or FPGC).
97% of SPSS enrollees do not pay based on financial
status.
Payment of providers in the public sector
are paid on a salary basis through the
institution they work for
Payment of providers in the private sector
are paid on a fee-for-service basis
In the public sector, wages are based on
seniority and vary between institutions who
care for the uninsured as well as those
providing care to those with Social Security
Most healthcare providers, specifically
doctors, rank among some of the lowest
salaries when compared to the average
income in Mexico
Low wages reduce the incentives for
providers to remain in healthcare or to pick
up a second job outside of the healthcare
profession
Current World Health Organization
(WHO) Ranking: # 61
WHO top causes of Death:
Diabetes
Ischemic Heart Disease
Stroke
Interpersonal violence
Cirrhosis of the Liver
COPD
Lower respiratory tract infections
Hypertensive heart disease
Road injury
Kidney diseases
MEXICO’S HEALTHCARE SYSTEM
Worthy Walker, MSN, FNP-BC; Ashley York MSN, AGNP-BC, WHNP-C; Cory York, BSN, SRNA
Faculty Advisor: Shari Wherry, DNP, APRN, FNP-C
Union University School of Nursing, Jackson, Tennessee
Financing for healthcare occurs through the following
ways in Mexico:
Social Security funded by payroll contributions from
federal government, employers, employees, and a
subsidy from the state.
SPSS publicly subsidized, funded by federal and state
government (All from general government revenues).
Federal: Social Contribution & Federal Solidarity
Contribution
States: Individual contribution (State Solidarity
Contribution)
Private funding is all out-of-pocket.
reimbursement for healthcare services occurs in two
ways:
The public sector sets annual global budgets
Private sectors arrange fee-for-service as the
predominant reimbursement service
Expenditure Total % of GDP (2013) 6.24
Expenditure, public % of government (2013) 15.38
Per Capita US dollar (2013) 664.34
Expenditure, private % of GDP in Mexico (2013) 3.01
Expenditure, public % of total health) (2013) 51.74
Hospital beds (per 1;000 people) (2009) 1.6
Physicians (per 1;000 people) (2009) 1.96
Nurses and midwives (1;000 people) (2000) 1.1
Outpatient visits per capita (2000) 2.5
Life Expectancy (in years) 75
MEXICAN POPULATION RESOURCES
Mexico has the 3rd largest population per country behind
the United States and Japan
In 2011, only 14 (5.1%) out of 273 Federal Programs and
Actions for Social Development were aimed at the
indigenous population
0.1% of GDP allocated to total national social policy
25% of the Mexican population reported having no health
insurance coverage
In 2002, 41 million Mexicans had Social Security
insurance coverage while 52 .5 million qualified for this
same coverage.