More Related Content
Similar to Accident Investigation Report 2013
Similar to Accident Investigation Report 2013 (20)
Accident Investigation Report 2013
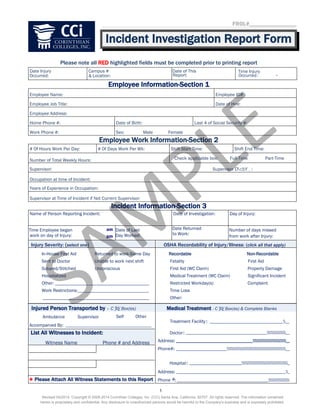
- 1. Incident Investigation Report Form.
Please note all RED highlighted fields must be completed prior to printing report
Date Injury
Occurred:
Campus #
& Location:
Date of This
Report:
Time Injury
Occurred:
Employee Information-Section 1
Employee Name: Employee ID#:
Employee Job Title: Date of Hire:
Employee Address:
Home Phone #: Date of Birth: Last 4 of Social Security #:
Work Phone #: Sex: Male Female
Employee Work Information-Section 2
# Of Hours Work Per Day: # Of Days Work Per Wk: Shift Start Time: Shift End Time:
Number of Total Weekly Hours: Check applicable box: Full-Time Part-Time
Supervisor:
Occupation at time of Incident:
Years of Experience in Occupation:
Supervisor at Time of Incident if Not Current Supervisor:
Incident Information-Section 3
Name of Person Reporting Incident: Date of Investigation: Day of Injury:
Time Employee began
work on day of Injury:
Date of Last
Day Worked:
Date Returned
to Work:
Number of days missed
from work after Injury:
Injury Severity: (select one) OSHA Recordability of Injury/Illness: (click all that apply)
In-House First Aid Returned to work-Same Day
Sent to Doctor Unable to work next shift
Sutured/Stitched Unconscious
Hospitalized
Other: _____________________________________________
Work Restrictions:__________________________________
___________________________________________________
Recordable Non-Recordable
Fatality First Aid
First Aid (WC Claim) Property Damage
Medical Treatment (WC Claim) Significant Incident
Restricted Workday(s) Complaint
Time Loss
Other:
Injured Person Transported by – C Box(es)
Ambulance Supervisor Self Other
Accompanied By: _________________________________________
Medical Treatment - C Box(es) & Complete Blanks
Treatment Facility : ___________________________________ __
Doctor: _______________________________________ __
Address: _____________________________________ __
Phone#: _________________________ __
Hospital: _________________________ _
Address: _____________________________________________________ _
Phone #: ____________________________________________
List All Witnesses to Incident:
Witness Name Phone # and Address
* Please Attach All Witness Statements to this Report
FROL#____________________
am
pm
Supervisor :
1
Revised 04/2014. Copyright © 2008-2014 Corinthian Colleges, Inc. (CCi) Santa Ana, California, 92707. All rights reserved. The information contained
herein is proprietary and confidential. Any disclosure to unauthorized persons would be harmful to the Company's business and is expressly prohibited.
SAM
PLE
- 2. Incident Investigation Report..
Investigation Information – Section 4
Exact Location of Incident:
Incident/Injury Reported To:
Sequence of Events: (Describe what happened before, during & after the incident)
(1) injured at the time ?
(2) The employee’s position relative to their immediate surroundings
(3) How was the employee doing what they were doing?
(4) What triggered the accident?
(5) type of accident that occurred and the cause
(6) Has the employee received any kind of treatment on this body part in the past? Yes No
_________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________ _
________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________ _
_______________________________________________________________________________________________________________ _
____________________________________________________________________________________________________________ __
____________________________________________________________________________________________________________ ____
If yes on #(6) describe:
Nature of Injury – Click Box(es)
Allergies/Sensitivities
Foreign Body-Eye
Amputation
Foreign Body-Other than Eye
Asphyxiation
Fracture
Bite/Sting
Hearing Loss
Bruise/Contusion
Heart Condition
Burn-Chemical
Hernia/Rupture
Burn-Contact
Infection
Burn-Electrical
Inflammation/Irritation
of Joints,Tendons or Muscles
Burn-Flame
Internal Bleeding
Carpal Tunnel Syndrome
Nervous System
Concussion
Pneumoconiosis
Concussionw/Unconsciousness
Poisoning
Contagious Conditions
Respiratory Conditions
Contusion
Scratch/Abrasion/Rash
Cut,Puncture,Open Wound
Sprains/Strains
Crush
Joints/Muscles/Tendons
Dislocation
____________________________
Stress, Mental
Disorders Associated
_________________________
w/Repeated Trauma
Multiple Injuries:
Electric Shock __________________
Excess Heat/Cold
___________________ __
CLICK BOX(ES) of AFFECTED BODY PART(S)
____________________________________________________________________________________________________________ ____
____________________________________________________________________________________________________________ ____
____________________________________________________________________________________________________________ ____
____________________________________________________________________________________________________________ ____
___________________ __
Multiple Head/Face Brain Head
Scalp
Eye(s)
Mouth/Nose
Neck
Skull
Face
Ear(s)
Teeth
ShoulderShoulder
Upper Back Upper Back
Upper Arm Upper Arm
Chest Chest
ElbowElbow
Sides/Ribs Sides/Ribs
Lower Back Lower Back
Abdomen Abdomen
Forearm Forearm
Wrist Wrist
Hand Hand
Finger(s) Finger(s)
Thigh Thigh
Hip(s) Hip(s)
Groin Groin
Knee Knee
Lower Leg Lower Leg
Ankle Ankle
Foot Foot
Toe(s) Toe(s)
L
E
F
T
S
I
D
E
O
F
B
O
D
Y
R
I
G
H
T
S
I
D
E
O
F
B
O
D
Y
____________________________________________________________________________________________________________ __
_________________________________________________________________________________________________________________
2
Revised 04/2014. Copyright © 2008-2014 Corinthian Colleges, Inc. (CCi) Santa Ana, California, 92707. All rights reserved. The information contained
herein is proprietary and confidential. Any disclosure to unauthorized persons would be harmful to the Company's business and is expressly prohibited.
SAM
PLE
- 3. Incident Investigation Report..
Safety Coordinator's Investigation Information – Section 5
Job Task – Click all Box(es) that apply Unsafe Condition(s) – Click Box(es) Unsafe Act(s) – Click Box(es)
Ascending/Descending:
Clean Up:
Other:____________________
Forklift:
Material Handling:
Maintenance:
MaintenanceOther:
Car/Truck:
Supervisory Task:
Tools: Hand Powered
Walking:
Other:
Workspace Conditions:
Environment:
Inside/Outside Lighting Conditions:
Equipment:
Fire:
Guard/Barrier:
Housekeeping:
Protective Equipment:
Protruding Object(s):
Storage:
Substance:
Surface:
Tool(s):
Training:
Warning System:
Other:______________________________________
Other:__________________
Other:__________________
Office Tasks:
Stair(s) Ladder(s) Vehicle
Equipment
General Outside
Adjusting
Operating Clearing Clearing Jam
Repairing
Operating Repairing
Pushing Pulling Powered
Vehicle Electrical
Hydraulic Mechanical
Loading Unloading
Restocking Moving
Enter Work Through Area
Exit Work
Filing Typing
(Repetitive)
Bending/Stooping
Sun Rain Snow
Severe
InadequateNone
Non-GivenInadequate
Defective Not-Available
Slipping
Hazard
Tripping
Hazard
Hazardous Non-Hazardous
Inadequate Improper
Good Fair Poor
Sharp
Object
Sharp
Surface
Improper Defective Inadequate
Fair Poor
Missing/
Not Installed Inadequate
Explosion Hazard
Modified Exposed/Energized
Defective Failure
Good Fair Poor
Noise Gasses/Fumes/Etc
Cold Temp Hot Temp
Congested Restricted
Please Include Any Pictures/Video Pertaining To The Incident/Accident
Clothing/Footwear(Other than P.P.E.)
Cell Phone Use
Bypassed - Guard/Barrier
Bypassed - Safety Device
Disregard Instructions
Disregard Rules
Driving Actions
Drugs or Alcohol
Equipment Operator Actions
Excessive Speed
Failure - Lockout/Tagout
Failure - To Obtain Assistance
Failure - To Secure
Failure - To Use P.P.E.
Failure - To Warn
Horseplay/Distraction
Impairment - Physical
Improper Lifting
Improper Loading or Stacking
Improper Placement or Storage
Improper Pushing or Pulling
Inattention to Surroundings
Incorrect Method
Intentional Act/Sabotage
Lack of Knowledge
Lack of Training
Need for Assistance
Positioning for Task
Other: _______________________
Office Equipment:
Supplies: Parking Lot Conditions:
Weather Conditions:
3
Revised 04/2014. Copyright © 2008-2014 Corinthian Colleges, Inc. (CCi) Santa Ana, California, 92707. All rights reserved. The information contained
herein is proprietary and confidential. Any disclosure to unauthorized persons would be harmful to the Company's business and is expressly prohibited.
SAM
PLE
- 4. Incident Investigation Report..
Investigation Information – Section 6
Personal Protective Equipment Required for Job Task– Click Box(es)
Hard Hat Respiratory Protection Gloves
Safety BeltHearing Protection Goggles Apron
Seat BeltSafety Glasses Face Shield Coveralls
Other:
PPE Availability – Click Box
Adequate Inadequate Improperly Used Not Available
Safety Rules – Click Box(es)
Adequate Inadequate None Not Enforced Other:__ ________________ _________
Training & Job Safety Analysis – Click Box(es)
Was there a safety orientation on this position? Yes No
Is there a Job Safety Analysis on this job? Yes No
If yes, was the Job Safety Analysis adequate? Yes No If no, has one been ordered? Yes No
If not adequate, has a revision been ordered? Yes No
Actions to Prevent Accident Recurrence - Click Box(es)
Action to improve design
Action to Improve Construction
Improved clean-up procedures
Improved lighting
Improved inspection procedures
Ordered Job Safety Analysis done
Ordered revision of Job Safety Analysis
Correction other than above:
_____________________________________________________________________________________________________________________ ____
Re- Instruct of employee(s) involved
Reprimand of employee(s) involved
Re- Instruct of others doing job
Temporary reassignment of Emp(s)
Permanent reassignment of Emp(s)
Correction of unnecessary congestion
Implement safety rule
Give new instructions
Inform all supervision
Improved noise/vibration control
Improved Personal Protective Equip.
Improved storage
Improved temperature control
Installation of guard or safety device
Tool/equipment repair/replacement
Use of safer materials/supplies
Corrective Actions / Fill in any Corrective Actions
Any Corrective Actions Person Responsible Completion Date
Required Signatures :
Employee Name:________________________________________ Signature:_________________________________________ _ Date:_____________
Supervisor Name:____________________________________ ___ Signature:_________________________________________ _ Date:_____________
Safety Coord. Name:_____________________________________ Signature:_________________________________________ _ Date:_____________
___________________________
___________________________
___________________________
Rolling Cart
4
Revised 04/2014. Copyright © 2008-2014 Corinthian Colleges, Inc. (CCi) Santa Ana, California, 92707. All rights reserved. The information contained
herein is proprietary and confidential. Any disclosure to unauthorized persons would be harmful to the Company's business and is expressly prohibited.
SAM
PLE