Wheel chair assessment Form
•Download as DOC, PDF•
5 likes•10,058 views

This document provides a wheelchair assessment form for collecting information about a patient's medical history, physical abilities, and needs for wheelchair seating and mobility equipment. The form collects details on diagnosis, posture, range of motion, strength, sensation, skin integrity, functional mobility, communication abilities, and environmental factors. Measurement data and photos are also included. Recommendations are made for specific wheelchair components to meet the patient's needs and facilitate independence.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (18)
Recently uploaded
Recently uploaded (20)
Wheel chair assessment Form
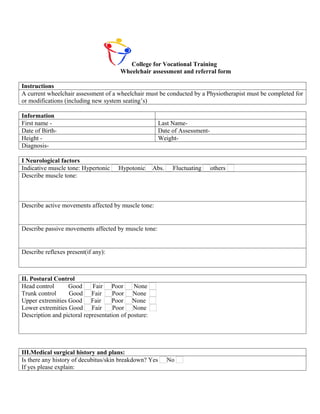
- 1. College for Vocational Training Wheelchair assessment and referral form Instructions A current wheelchair assessment of a wheelchair must be conducted by a Physiotherapist must be completed for or modifications (including new system seating’s) Information First name - Last Name- Date of Birth- Date of Assessment- Height - Weight- Diagnosis- I Neurological factors Indicative muscle tone: Hypertonic Hypotonic Abs. Fluctuating others Describe muscle tone: Describe active movements affected by muscle tone: Describe passive movements affected by muscle tone: Describe reflexes present(if any): II. Postural Control Head control Good Fair Poor None Trunk control Good Fair Poor None Upper extremities Good Fair Poor None Lower extremities Good Fair Poor None Description and pictoral representation of posture: III.Medical surgical history and plans: Is there any history of decubitus/skin breakdown? Yes No If yes please explain:
- 2. Describe orthopedic conditions and/ or range of motion requiring special consideration (i.e., contractures, degree of spinal curvature, etc.): Describe other physical limitation or concerns (i.e., respiratory): Describe any recent changes in medical/Physical/functional status: Brief description if the child/adult has undergone any surgery: IV. Functional assessment Ambulatory status: Non ambulatory With assistance Short distance only Community ambulatory Description: Indicate the child’s /adults ambulatory potential: Already using a wheel chair Expected in 1 year Not expected Expected in future __ Years. Description: IV. Functional assessment: Is the child/adult totally dependent on W/C? Yes No If No, please explain: Indicate the child/adults transfer capacities: Maximum assistance Moderate assistance Minimum assistance None Notes: Is the child/adult tube fed? Yes No If yes please explain: Feeding: Maximum assistance Moderate assistance Minimum assistance None Notes:
- 3. Dressing: Maximum assistance Moderate Minimum assistance None Notes: He needs full assistance in dressing and undressing. Describe the activities performed in wheelchair: (Mobility,feeding,socializing with peers, school, home, family, engaging in community activity) TRANSPORTATION: Car Van Bus Bike Other : Sits in wheelchair during transport Where is w/c stored during transport? Tie Downs Self Driver Drive while in Wheelchair yes no Employment: Specific requirements pertaining to mobility School: Specific requirements pertaining to mobility Other: FUNCTIONAL/SENSORY PROCESSING SKILLS: Handedness: Right Left NA Comments: Functional Processing Skills for Wheeled Mobility Processing Skills are adequate for safe wheelchair operation Comments: COMMUNICATION: Verbal Communication WFL receptive WFL expressive Difficult to understand non-communicative Uses an augmentative communication device AAC Mount Needed: SENSATION and SKIN ISSUES: Sensation Pressure Relief: Intact Impaired Absent Able to perform effective pressure relief : Yes No Hyposensate Hypersensate Method: If not, Why?: Defensiveness Level of sensation: Skin Issues/Skin Integrity Current Skin Issues Yes No History of Skin Issues Yes Hx of skin flap surgeries Yes No Intact Red area Open Area No Where ________________________ Where When _________________________ Scar Tissue At risk from prolonged sitting Where ___________________________ ________________________ When _________________________
- 4. Complaint of Pain: Please describe ADL STATUS (in reference to wheelchair use): Indep Assist Unable Indep Not Comments with assessed Equip Dressing Eating Describe oral motor skills Grooming/Hygiene Meal Prep IADLS Comments: Bowel Mngmnt: Continent Incontinent Accidents Comments: Bladder Mngmnt: Continent Incontinent Accidents CURRENT SEATING / MOBILITY: Current Mobility Base: None Dependent Dependent with Tilt Manual Scooter Power Type of Control: Current Condition of Mobility Base: Current Seating System: Age of Seating System: COMPONENT MANUFACTURER/CONDITION Seat Base Cushion Back Lateral trunk supports Thigh support Knee support Foot Support Foot strap Head Support Pelvic Stabilization Anterior Chest/Shoulder Support UE Support Other When relevant: Overall seat height Overall w/c length Overall w/c width Describe posture in present seating system: V. Environmental assessment Describe the place where Wheel chair is going to be used(home/school):
- 5. Is the home/School accessible for W/C? Yes No Are there ramps in home/School? Yes No Needs modification RECOMMENDATION / GOALS : MANUAL WHEELCHAIR POV POWER WHEELCHAIR: POSITIONING SYSTEM(TILT/RECLINE) SEATING WHEELCHAIR SKILLS: Indep Assist Dependent/ N/A Comments unable Bed ↔ w/c Chair Transfers w/c ↔ Commode Transfers Manual w/c Propulsion: UE or LE strength and Arm : left right Both endurance sufficient to participate in Foot: left right Both ADLs using manual wheelchair Operate Scooter Strength, hand grip, balance , transfer appropriate for use. Living environment appropriate for scooter use. Operate Power w/c: Std. Joystick Safe Functional Distance Operate Power w/c: w/ Alternative Controls Safe Functional Distance MOBILITY/BALANCE: Balance Transfers Ambulation Sitting Balance: Standing Balance Independent Independent WFL WFL Min Assist Ambulates with Asst Uses UE for balance in sitting Min assist Mod Asst Ambulates with Device Min Assist Mod assist Max assist Indep. Short Distance Only Mod Assist Max assist Dependent Unable to Ambulate Max Assist Unable Sliding Board Unable Lift / Sling Required Comments:
- 6. MAT EVALUATION : A F G C H B I D J K L E M N O Measurements in Sitting: Left Right A: Shoulder Width B: Chest Width H: Seat to Top of Shoulder C: Chest Depth (Front – Back) I: Acromium Process (Tip of Shoulder) D. Hip width J: Inferior Angle of Scapula E. Between Knees K: Seat to Elbow F. Top of Head L: Seat to Iliac Crest G. Occiput M: Upper leg length ++ Overall width (asymmetrical width for N: Lower leg length windswept legs or scoliotic posture O: Foot Length Additional Comments: Hamstring flexibility: Pelvis to thigh angle accommodate greater than 90 Thigh to calf angle accommodate less than 90 Describe Reflexes/tonal influence on body:
- 7. COMMENTS: POSTURE: Anterior / Posterior Obliquity Rotation-Pelvis P E L V I Neutral Posterior WFL R elev l elev WFL Right Left S Anterior Anterior Anterior Fixed Other Fixed Other Fixed Other Partly Flexible Partly Flexible Partly Flexible Flexible Flexible Flexible TRUNK Rotation-shoulders and upper Anterior / Posterior Left Right trunk Neutral WFL ↑ Thoracic ↑ WFL Convex Convex Left-anterior Lumbar Kyphosis Left Right-anterior Lordosis Right c-curve s-curve multiple Fixed Flexible Fixed Flexible Fixed Flexible Partly Flexible Other Partly Flexible Partly Flexible Other Other Describe LE Neurological Influence/Tone: Position Windswept Hip Flexion/Extension Limitations: H I P S Neutral Abduc ADduct Neutral Right Left
- 8. Fixed Fixed Other Subluxed Partly Flexible Partly Flexible Hip Internal/External Dislocated Range of motion Limitations: Flexible Flexible Knee R.O.M. Foot Positioning Left Right WFL L R KNEES WFL WFL ROM concerns: & Limitations Dorsi-Flexed L R Limitations FEET Plantar Flexed L R Inversion L R Eversion L R COMMENTS: Posture: Good Head Control Describe Tone/Movement HEAD of head and Neck: Functional & Flexed Extended Adequate Head Control Rotated L Lat Flexed Limited Head Control NECK L Rotated R at Flexed R Cervical Hyperextension Absent Head Control Upper R.O.M. for Upper Describe Extremity SHOULDERS Extremity Tone/Movement of UE: WNL WFL Limitations: Left Right Functional Functional elev / dep elev / dep UE Strength Concerns: pro-retract pro- N/A retract None subluxed subluxed Concerns: R.O.M. ELBOWS Left Right
- 9. Strength concerns: Left Right Strength / Dexterity: WRIST & Fisting HAND Goals for Wheelchair Mobility Independence with mobility in the home and motor related ADLs (MRADLs) in the community Independence with MRADLs in the community Provide dependent mobility Provide recline Provide tilt Goals for Seating system Optimize pressure distribution Provide support needed to facilitate function or safety Provide corrective forces to assist with maintaining or improving posture Accommodate client’s posture: current seated postures and positions are not flexible or will not tolerate corrective forces Client to be independent with relieving pressure in the wheelchair Enhance physiological function such as breathing, swallowing, digestion Simulation ideas: Equipment trials: State why other equipment was unsuccessful: SEATING COMPONENT RECOMMENDATIONS AND JUSTIFICATION Component Manuf/mod/size Justification Seat Cushion accommodate impaired stabilize pelvis sensation accommodate obliquity decubitus ulcers present accommodate multiple prevent pelvic extension deformity low maintenance neutralize LE increase pressure
- 10. distribution Seat Wedge accommodate ROM Provide increased aggressiveness of seat shape to decrease sliding down in the seat Cover Replacement protect back or seat cushion Mounting fixed attach seat platform/cushion to mount headrest hardware w/c frame swing medial thigh lateral trunk supports swing away for: attach back cushion to w/c support away headrest frame swing lateral supports away for transfers medial thigh support back seat Seat Board support cushion to prevent allows attachment of Back Board hammocking cushion to mobility base Back provide lateral trunk support provide posterior trunk accommodate deformity support accommodate or decrease tone provide lumbar/sacral support facilitate tone support trunk in midline Lateral pelvic/thigh pelvis in neutral accommodate tone support removable for transfers accommodate pelvis position upper legs Medial Knee decrease adduction remove for transfers Support accommodate ROM alignment Foot Support position foot stability accommodate deformity decrease tone control position Ankle strap/heel support foot on foot support provide input to heel loops decrease extraneous protect foot movement Lateral trunk R L decrease lateral trunk leaning safety Supports accom asymmetry control of tone contour for increased contact Anterior chest decrease forward movement of added abdominal strap, vest, or shoulder support shoulder retractors accommodation of TLSO alignment decrease forward movement of assistance with shoulder trunk control decrease shoulder elevation Component Manuf/mod/size Justification Headrest provide posterior head support improve respiration
- 11. provide posterior neck support placement of switches provide lateral head support safety provide anterior head support accommodate ROM support during tilt and recline accommodate tone improve feeding improve visual orientation Neck Support decrease neck rotation decrease forward neck flexion Upper R L decrease edema decrease gravitational pull on Extremity decrease subluxation shoulders Support control tone provide midline positioning Arm trough provide work surface provide support to increase Posterior hand UE function placement for support AAC/Computer/EADL provide hand support in natural ½ tray position full tray swivel mount Pelvic stabilize tone pad for protection over boney Positioner decrease falling out of chair/ prominence Belt **will not decrease potential for prominence comfort SubASIS bar sliding due to pelvic tilting special pull angle to control prevent excessive rotation rotation Dual Pull Bag or pouch Holds: diapers catheter/hygiene medicines special food ostomy supplies orthotics clothing changes Other
- 12. Recommendations/ Modifications in the W/C: Signature of the PT