ICH stroke guidelines 2015 summary - surgical & blood pressure management
•
6 likes•4,237 views

Baru saja diterbitkan guideline manajemen stroke ICH 2015 oelh AHA/ASA, meng-update guideline sebelumnya yang dirilis tahun 2010. Penasaran, saya langsung lompat ke bagian manajemen blood pressure & surgical treatment (membandingkan dengan guideline 2010, guideline yang diterbitkan Eropa dan Korea tahun 2014), dan ternyataaa.... (Tunggu aja info lengkapnya, akan diuraikan di: https://neurobsession.wordpress.com/2015/08/02/intracerebral-hemorrhage-stroke-guidelines-2015-the-enigma/ --mungkin lebih seperti "curhat" sih jadinya..) Yak, selamat membaca!

Recommended
More Related Content
More from Ersifa Fatimah
More from Ersifa Fatimah (20)
Recently uploaded
Recently uploaded (20)
ICH stroke guidelines 2015 summary - surgical & blood pressure management
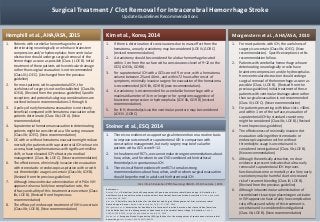
- 1. 1. For most patients with ICH, the usefulness of surgery is uncertain (Class IIb; LOE C). (New recommendation). Specific exceptions to this recommendation follow. 2. Patients with cerebellar hemorrhage who are deteriorating neurologically or who have brainstem compression and/or hydrocephalus from ventricular obstruction should undergo surgical removal of the hemorrhage as soon as possible (Class I; LOE B). (Revised from the previous guideline) Initial treatment of these patients with ventricular drainage alone rather than surgical evacuation is not recommended (Class III; LOE C). (New recommendation) 3. For patients presenting with lobar clots >30mL and within 1 cm of the surface, evacuation of supratentorial ICH by standard craniotomy might be considered (Class IIb; LOE B). (Revised from the previous guideline) 4. The effectiveness of minimally invasive clot evacuation utilizing either stereotactic or endoscopic aspiration with or without thrombolytic usage is uncertain and is considered investigational (Class IIb; LOE B). (New recommendation) 5. Although theoretically attractive, no clear evidence at present indicates that ultra-early removal of supratentorial ICH improves functional outcome or mortality rate. Very early craniotomy may be harmful due to increased risk of recurrent bleeding (Class III; LOE B). (Revised from the previous guideline) 6. Although intraventricular administration of recombinant tissue-type plasminogen activator in IVH appears to have a fairly low complication rate, efficacy and safety of this treatment is uncertain and is considered investigational (Class IIb; LOE B). (New recommendation) 1. If there is deterioration of consciousness due to mass effect from the hematoma, an early craniotomy may be considered (LOE IV, GOR C) (revised recommendation). 2. A craniotomy should be considered for a lobar hemorrhage located within 1 cm from the surface with a consciousness level of 9–12 on the GCS (LOE IIb, GOR B). 3. For supratentorial ICH with a GCS score of 9 or over, with a hematoma volume between 25 and 40 mL, and within 72 hours after onset of symptoms, minimally invasive surgery for evacuation of the hematoma is recommended (LOE IIb, GOR B) (new recommendation). 4. A craniotomy is recommended for a cerebellar hemorrhage with a maximal diameter of 3 cm or longer or for symptoms suggestive of brainstem compression or hydrocephalus (LOE IIb, GOR B) (revised recommendation). 5. For IVH, thrombolysis via the ventricular puncture may be considered (LOE IV, GOR C) 1. Patients with cerebellar hemorrhage who are deteriorating neurologically or who have brainstem compression and/or hydrocephalus from ventricular obstruction should undergo surgical removal of the hemorrhage as soon as possible (Class I; LOE B). Initial treatment of these patients with ventricular drainage rather than surgical evacuation is not recommended (Class III; LOE C). (Unchanged from the previous guideline) 2. For most patients with supratentorial ICH, the usefulness of surgery is not well established (Class IIb; LOE A). (Revised from the previous guideline) Specific exceptions and potential subgroup considerations are outlined below in recommendations 3 through 6. 3. A policy of early hematoma evacuation is not clearly beneficial compared with hematoma evacuation when patients deteriorate (Class IIb; LOE A). (New recommendation) 4. Supratentorial hematoma evacuation in deteriorating patients might be considered as a life-saving measure (Class IIb; LOE C). (New recommendation) 5. DC with or without hematoma evacuation might reduce mortality for patients with supratentorial ICH who are in a coma, have large hematomas with significant midline shift, or have elevated ICP refractory to medical management (Class IIb; LOE C). (New recommendation) 6. The effectiveness of minimally invasive clot evacuation with stereotactic or endoscopic aspiration with or with- out thrombolytic usage is uncertain (Class IIb; LOE B). (Revised from the previous guideline) 7. Although intraventricular administration of rtPA in IVH appears to have a fairly low complication rate, the effcacy and safety of this treatment are uncertain (Class IIb; LOE B). (Revised from the previous recommendation) 8. The efficacy of endoscopic treatment of IVH is uncertain (Class IIb; LOE B). (New recommendation) Surgical Treatment / Clot Removal for Intracerebral Hemorrhage Stroke Update Guidelines Recommendations Hemphill et al., AHA/ASA, 2015 Kim et al., Korea, 2014 Morgenstern et al., AHA/ASA, 2010 References: Hemphill et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage : A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke, published online May 28, 2015. Kim et al. Clinical Practice Guidelines for the Medical and Surgical Management of Primary Intracerebral Hemorrhage in Korea. J Korean Neurosurg Soc 56 (3) : 175-187, 2014 Morgenstern et al. Association for Healthcare Professionals From the American Heart Association/American Stroke Guidelines for the Management of Spontaneous Intracerebral Hemorrhage : A Guideline. Stroke. 2010;41:2108-2129; originally published online July 22, 2010. Steiner et al. European Stroke Organisation (ESO) guidelines for the management of spontaneous intracerebral hemorrhage. Int J Stroke. 2014 Oct;9(7):840-55. Divisi Ilmiah Kelurahan PPDS Neurologi UNAIR – RS Dr Soetomo | 2015 1. There is no evidence to support surgical intervention on a routine basis to improve outcome after supratentorial ICH in comparison with conservative management, but early surgery may be of value for patients with a GCS score 9–12. 2. In the absence of RCTs, we cannot make strong recommendations about how, when, and for whom to use EVD combined with intrathecal thrombolysis in spontaneous ICH. 3. There is insufficient evidence from RCTs to make strong recommendations about how, when, and for whom surgical evacuation should be performed in adults with infratentorial ICH. Steiner et al., ESO, 2014
- 2. 1. The suggested BP targets in patients with acute ICH are described below (LOE III, GOR B). Drugs that can be used for BP control in spontaneous ICH are shown in Table 2 (revised recommendation). 1) If the SBP is >200 mm Hg or MAP is >150 mm Hg, then consider aggressive BP reduction with a continuous intravenous infusion of drugs, with frequent BP monitoring every 5 minutes. 2) If the SBP is >180 mm Hg or MAP is >130 mm Hg and there is any possibility of an ICP elevation, then consider ICP monitoring and reducing BP using an intermittent or continuous intravenous infusion while maintaining a CPP (MAP-ICP) of 50–70 mm Hg. 3) If the SBP is >180 mm Hg or MAP is >130 mm Hg and there is no evidence of an ICP elevation, then consider a modest reduction of BP using an intermittent or continuous intravenous infusion (MAP of 110 mm Hg for a BP of 160/90 mm Hg) and clinically re-examine the patient every 15 minutes. 2. In patients with acute ICH, when the SBP is measured between 150 and 220 mm Hg, the SBP may be safely lowered to 140 mm Hg within 1 hour (LOE Ib, GOR A) (new Recommendation). Intracerebral Hemorrhage Stroke - The Management of Blood Pressure Update Guideline Recommendations 1. For ICH patients presenting with SBP between 150 and 220 mm Hg and without contraindication to acute BP treatment, acute lowering of SBP to 140 mm Hg is safe (Class I; Level of Evidence A) and can be effective for improving functional outcome (Class IIa; Level of Evidence B). (Revised from the previous guideline) 2. For ICH patients presenting with SBP >220 mm Hg, it may be reasonable to consider aggressive reduction of BP with a continuous intravenous infusion and frequent BP monitoring (Class IIb; Level of Evidence C). (New recommendation) Kim at al., Korea, 2014 1. Until ongoing clinical trials of BP intervention for ICH are completed, physicians must manage BP on the basis of the present incomplete efficacy evidence. Current suggested recommendations for target BP in various situations are listed in Table 6 and may be considered (Class IIb; LOE C). (Unchanged from the previous guideline) 2. In patients presenting with a systolic BP of 150 to 220 mmHg, acute lowering of systolic BP to 140 mmHg is probably safe (Class IIa; LOE B). (New recommendation) Hemphill et al., AHA/ASA, 2015 Morgenstern et al., AHA/ASA, 2010 References: Hemphill et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage : A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke, published online May 28, 2015. Kim et al. Clinical Practice Guidelines for the Medical and Surgical Management of Primary Intracerebral Hemorrhage in Korea. J Korean Neurosurg Soc 56 (3) : 175-187, 2014 Morgenstern et al. Association for Healthcare Professionals From the American Heart Association/American Stroke Guidelines for the Management of Spontaneous Intracerebral Hemorrhage : A Guideline. Stroke. 2010;41:2108-2129; originally published online July 22, 2010. Steiner et al. European Stroke Organisation (ESO) guidelines for the management of spontaneous intracerebral hemorrhage. Int J Stroke. 2014 Oct;9(7):840-55.Divisi Ilmiah Kelurahan PPDS Neurologi UNAIR – RS Dr Soetomo | 2015 In acute ICH within 6 h of onset, intensive blood pressure reduction (systolic target <140 mmHg in <1h) is safe and may be superior to a systolic target <180 mmHg. No specific agent can be recommended. Steiner et al., ESO, 2014