1. Without BordersMédecins Sans Frontières/Doctors Without Borders | msf.org.uk
Ebola is one of
the world’s most
deadly diseases.
The virus can kill
up to 90 percent
of the people who
catch it. Ebola is
so infectious that
patients need to be treated in
isolation by staff wearing special
protective clothing. MSF has
launched an emergency response
to combat an Ebola outbreak
in west Africa, which has
claimed hundreds of lives. MSF
epidemiologist Michel Van Herp
reports on efforts to combat this
terrifying disease.
Ireceived a message at home about
this strange disease which had
broken out in southern Guinea. They
thought that perhaps it was Lassa fever,
but when I received a description of the
patients’ symptoms, it was clear to me
we were talking about Ebola. A couple
of days later I was in Guinea.
‘It’s like detective work’
I’ve worked in every major outbreak of
Ebola since 2000. What makes this one
different is its geographical spread, which is
unprecedented. There are cases in at least six
towns in Guinea, as well as across the border
in Liberia.
The problem is that everybody moves around
– infected people move from one village to
another while they’re still well enough to walk;
even the dead bodies are moved from place
to place. Tracking the disease is like doing
detective work.
continued on page 2
Ebola: fighting
the killer virus
MSF staff at our Ebola treatment
centres in Guinea and Sierra
Leone risk infection to treat
hundreds of patients each month.
But they can’t operate without
donations. Please support our
medical teams working around
the world today.
Phone: 0800 408 3894
Visit: www.msf.org.uk/support
Or use the form on page 3
INSIDE:
4-5 MSF FIGHTING EBOLA
6 CENTRAL AFRICAN REPUBLIC
7 THROUGH THE LENS
8 YEMEN
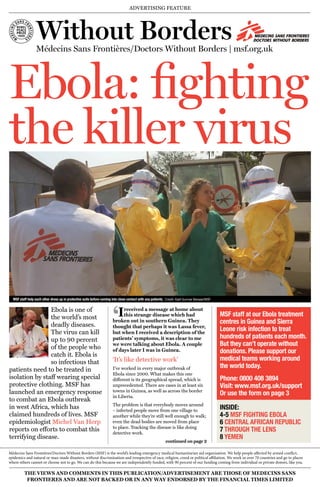
MSF staff help each other dress up in protective suits before coming into close contact with any patients. Credit: Kjell Gunnar Beraas/MSF
Médecins Sans Frontières/Doctors Without Borders (MSF) is the world’s leading emergency medical humanitarian aid organisation. We help people affected by armed conflict,
epidemics and natural or man-made disasters, without discrimination and irrespective of race, religion, creed or political affiliation. We work in over 70 countries and go to places
where others cannot or choose not to go. We can do this because we are independently funded, with 90 percent of our funding coming from individual or private donors, like you.
‘
ADVERTISING FEATURE
THE VIEWS AND COMMENTS IN THIS PUBLICATION/ADVERTISEMENT ARE THOSE OF MEDECINS SANS
FRONTIERES AND ARE NOT BACKED OR IN ANY WAY ENDORSED BY THE FINANCIAL TIMES LIMITED
2. EBOLA CRISIS SUPPORTING MSF
2 3
/msf.English @msf_uk
SUPPORT MAKES OUR WORK POSSIBLE + WE CAN’T OPERATE WITHOUT YOU + YOUR SUPPORT SAVES LIVES + YOUR
89%
on humanitarian work
8%
on fundraising
3%
on office management
!
!
Your support makes our work possible – thank you!
£10 a month – or 33p
a day – can help provide
an MSF team with an
emergency dressing
kit containing sterile
equipment, dressings and
bandages to help people
caught up in conflict.
£20 a month
can buy medicine to
treat 200 people for
malaria: a treatable
disease that kills one
child every 30 seconds.
Credit: Seb Geo Credit: Marcell Nimfuehr/MSF
The one thing we can’t do without is your
support. Regular support — such as a monthly
donation — means we can plan ahead,
confident that the funds we need will be there
when we need them. It means we don’t have to
waste money on administration that could be
spent on saving lives.
Giving monthly is easy for you too. No hassle. No
time wasting. Just your money getting to where
it’s needed, fast.
We can’t do it without you
I would like to make a monthly contribution of £10 £20
or my own choice of £__________
starting on 1st 15th 28th of M M / Y Y Y Y
alternatively MSF will claim on the next available date
Please allow four weeks for the Direct Debit to be set up.
PLEASE COMPLETE IN BLOCK CAPITALS (We will NOT pass your details to anyone else)
Title Forename
Surname
Address
Town Postcode
Please provide the following information if you would like to be contacted in any of
these ways:
Telephone
Mobile
Email address
Instruction to your Bank or
Building Society to pay by Direct Debit
Name(s) of Account Holders
Bank/Building Society Account Number
Sort Code – –
Name and full postal address of your Bank or Building Society:
To the Manager
Bank/Building Society
Address
Postcode
Instruction to your Bank or Building Society
Please pay Charity Pay Limited Re: MSF UK Direct Debits from the account detailed in this instruction subject to the
safeguards assured by the Direct Debit Guarantee. I understand that this instruction may remain with Charity Pay
Limited Re: MSF UK and if so, details will be passed electronically to my Bank/Building society.
Signature(s)
Today’s Date D D / M M / Y Y Y Y
Banks and Building Societies may not accept Direct Debit Instructions for some types of account. Charity Pay
Limited Re: MSF UK Direct Debits will show MSF UK on your bank statements.
Please return to: MSF UK, FREEPOST RTGZ-KUHJ-XHKU, MSFUK,
2A Halifax Road, Melksham,Wiltshire, SN12 6YY.
Alternatively phone 0800 408 3894 (open 24 hours a day 7 days a week)
or make your donation online at www.msf.org.uk/support
Charity Registration Number 1026588
Are you a UK taxpayer? If so, you can make your gift
worth more at no extra cost. Please tick the box below.
I wish Médecins Sans Frontières to treat all gifts in the last 4 years, this gift and all
future gifts that I make, as Gift Aid donations. I confirm I have paid or will pay an
amount of Income tax and/or Capital gains tax for each tax year, that is at least equal
to the amount of tax that all the charities and CASCs that I donate to will reclaim on
my gifts for that tax year. I understand that other taxes such as VAT and Council tax
do not qualify; and that the charity will reclaim 25p of tax on every £1 that I give.
Date: _______ /_______ /_______
Yes, I will support MSF’s
volunteer medical teams
Originator’s ID Number
2 8 5 6 8 2
Charity Pay Limited Re: MSF UK
CODE
OUR GUARANTEE TO YOU
We respect and value every one of
our supporters. We won’t allow any
other organisation to have access
to your name and address. Neither
will we send you constant appeals.
We do want to share the reality of
our work with you. When you give us
your details, you agree to receiving
information about our work and the
difference your support makes. If you
would prefer not to hear about us
please email anne.farragher@london.
msf.org, call 0207 067 4214 or write
to: Anne Farragher, Médecins Sans
Frontières, 67-74 Saffron Hill, London,
EC1N 8QX.
(For every £1 we spent on
fundraising in 2013, we raised £13)
We’re proud
of how we
spend your
contributions
MSF UK Annual Report 2012
There are three ways you can start supporting MSF’s lifesaving work today.
Make a regular monthly gift online at www.msf.org.uk/support
You can also call us free on 0800 408 3894 24 hours. Please have your bank details to hand.
Alternatively, you can complete the Direct Debit form below, place it in an envelope and
post it to: Médecins Sans Frontières, FREEPOST RTGZ-KUHJ-XHKU, MSFUK,
2A Halifax Road, Melksham, Wiltshire, SN12 6YY.
1
2
3
continued from front page
We’ve learned from our previous experiences
with Ebola that patients have a 10 to 15
percent better chance of survival if they receive
good medical support. But if they stay at
home, the fatality rate generally reaches up to
90 percent.
‘Fear is normal’
For health staff , it is normal to feel some kind
of fear when you enter the isolation area for
the first time, even if you are well protected.
But you follow a kind of ritual – for dressing
and undressing, and for all the activities
you perform inside – little by little, you gain
confidence.
You never enter the isolation area alone – you
always enter in pairs. And you only go in for
short periods, because it is very hot in Guinea
and even hotter inside the yellow protective
suits. It is tiring, especially if you are doing
physical work. We always write our names on
the front of our aprons so that the patients
know who is in front of them.
WHAT IS EBOLA?i
The Ebola virus is thought to live in fruit bats
and to spread to humans through contact
with sick animals. Highly infectious, the
disease is passed from person to person
through bodily fluids including saliva, sweat,
blood and semen. The current outbreak
involves the Zaire strain, which can kill up
to 90 percent of people infected. There is
no vaccine against Ebola, and no cure, but
good medical care can help patients develop
antibodies to fight the disease and can bring
the mortality rate down by 10 or 15 percent.
The Ebola virus is thought to live in fruit bats and to
spread to humans through contact with sick animals.
Highly infectious, the disease is passed from person to
person through bodily fluids including saliva, sweat,
blood and semen. The current outbreak involves the Zaire
strain, which kills up to 90 percent of people infected.
There is no vaccine against Ebola, and no cure, but good
medical care can help patients develop antibodies to
fight the disease and can bring the mortality rate down
by 10 or 15 percent.
Inside the centre, we try and make the patients
as comfortable as possible. Sometimes we
bring the parent of a sick person in to visit
them. They have to wear a protective suit with
a mask and goggles and gloves. The relatives
are supervised, so there is no possibility of any
contact with a patient’s bodily fluids.
Patients who are deeply affected by the disease
do not have a lot of energy to communicate.
The mood can be very sombre with those in a
terminal stage, who have only a few hours left
before they die.
When a patient dies, we put them in a special
body bag so that the burial can be done
WHAT IS MSF DOING?i
In recent weeks, further cases have been
reported in Guinea and in neighbouring
Sierra Leone. The virus has already
affected more than 300 people and MSF
is continuing its work supporting health
authorities in the two countries, treating
patients and putting measures in place to
contain the epidemic.
MSF has 300 staff on the ground and
has brought in more than 40 tonnes of
equipment and supplies to help fight the
epidemic. It’s the financial support of
individuals like you that enables us to do
this. Thank you.
For more information,
visit: msf.org.uk/ebola
according to family traditions. If the patient
comes from a village, we take the body back
and advise relatives about what they can do
– and what they should not be afraid to do –
during the funeral.
Once the body bag has been sprayed, it can be
handled with gloves, so the mourners can wear
their normal clothes to the funeral. We do not
steal the body from the family; we try to treat
it with dignity, and respect their traditions as
much as possible.
‘People can survive’
The mortality rate for Ebola is high, but there
are survivors. Just before I left Guinea, our
first two patients left the MSF centre cured of
the disease: Thérèse, 35, and Rose, 18. Both
are from the same extended family, which
had already seen seven or 10 deaths from the
disease.
Their relatives were overjoyed. There was
a huge celebration in the village when they
returned.
They come from a family of local healers, so
the news that they were cured will spread
to other villages, and I hope this will create
further trust.
People can survive; as the patients left, our
teams were cheering. To know that they
survived helps you forget all the bad things.
Physical contact and lots of talking help patients in the isolation zone feel less alone. Credit: Sylvain Cherkaoui/Cosmos
After ten days in the isolation zone, Ebola survivor Rose receives a farewell hug from the nurse who cared for her.
Credit: Amandine Colin/MSF
Sierra Leone
Guinea
Mali
Senegal
Côte d’Ivoire
Liberia
ADVERTISING FEATURE ADVERTISING FEATURE
3. EBOLA CRISIS
4 5
SUPPORT MAKES OUR WORK POSSIBLE + WE CAN’T OPERATE WITHOUT YOU + YOUR SUPPORT SAVES LIVES + YOURSUPPORT MAKES OUR WORK POSSIBLE + WE CAN’T OPERATE WITHOUT YOU + YOUR SUPPORT SAVES LIVES + YOUR
How we treat Ebola
When Ebola haemorrhagic fever broke out recently in Guinea, west Africa, MSF set up three specialised treatment centres in the worst-hit areas.
Ebola is so infectious – and so deadly – that patients need to be treated in isolation by staff wearing special protective clothing. Emergency
coordinator Henry Gray and logistician Pascal Piguet, both just back from Guinea, explain why, with Ebola, every little detail counts.
staff entrance
to high-risk zone
staff exit from
high-risk zone
high-risk zone
suspected cases
low-risk zone
high-risk zone
confirmed cases
triage tent
entrance for staff
entrance for
patients
exit for cured patients
treatment ward
treatment ward
showers latrines
showers latrines
laundry, showers
and latrines
water tank
pharmacy
changing area
office
stores
incinerator
meeting tent
ward
visitors’ area
ward
morgue
shower
5 Exit for cured patients
When a patient is feeling better
and has had two negative lab
tests in a row, they are allowed
home. Before leaving, they
shower in chlorinated water
and receive clean clothes and a
package containing therapeutic
food and vitamins to build up
their strength.
2 High-risk zone – confirmed cases
“The high-risk zone’s not an easy place
to be – you’re isolated, you’ve got no
access to the outside world. So we try
and make it as friendly as possible, with
a TV, radios, plastic chairs and shaded
areas to sit,” says Henry.
3 Treatment ward
“With a mortality rate of up to 90 percent,
we know that most people in the
treatment ward will not come out. We do
the most we can for them: whatever the
patient wants, the patient gets – special
food, new items of clothing... It’s easy to
do and it does them good,” says Pascal.
4 Visitors’ area
Family members talk with patients
through the fence, local religious
leaders offer moral support, and MSF
psychologists provide counselling.
2 Changing area
Before entering the high-risk zone, staff
help each other put on their protective
suits, while respecting the strict ‘no body-
to-body contact’ rule.
3 Staff entrance to high-risk zone
“Each time we go in, we have to plan it
down to the finest detail. To prepare, we
have a 30-minute briefing about what
we are going to do, and we get all the
equipment ready beforehand.” says Pascal.
4 Staff exit from
high-risk zone
On leaving the high-risk
area, staff remove their
protective suits and
disinfect themselves.
5 Laundry
All recyclable items of
clothing are washed
in chlorinated water
every day and
reused.
6 Incinerator
Everything used in
the high-risk area
which can’t be
disinfected is burnt.
1 Protective clothing
“The suits are so stifling that it’s hard to stay inside
for more than 40 minutes. You sweat a lot - up
to two litres each time - but you don’t cool down
because the sweat doesn’t evaporate,” says Pascal.
1 High risk zone – suspected cases
Many of the early symptoms of Ebola
are similar to diseases such as malaria
and TB. “It’s really important that there
are separate zones for suspected and
confirmed cases, because you don’t
want to contaminate someone with TB
with Ebola – that’s basically a death
sentence,” says Henry.
A lab test takes as little as four hours to
confirm the disease. Patients who test
positive are admitted to the zone for
confirmed cases.
Graphic: Natasha Lewer/Lou Lewer
Plastic goggles: £5.16
Protective mask: 67p
Protective
suit: £16.41
Chemical-
resistant
gloves: £2.66
Plastic apron: £4.05
Rubber boots: £9.22
YOUR SUPPORT
£38.17
pays for a complete protective suit for
an MSF staff member working in one of
the Ebola treatment centres in Guinea.
£
ADVERTISING FEATURE ADVERTISING FEATURE
4. CENTRAL AFRICAN REPUBLIC THROUGH THE LENS
6 7
SUPPORT MAKES OUR WORK POSSIBLE + WE CAN’T OPERATE WITHOUT YOU + YOUR SUPPORT SAVES LIVES + YOUR SUPPORT MAKES OUR WORK POSSIBLE + WE CAN’T OPERATE WITHOUT YOU + YOUR SUPPORT SAVES LIVES + YOUR
Central African Republic, April 2014 – A Muslim
resident of Bossangoa seeks safety from
Christian militias in the grounds of a school, in a
country that is being torn apart by intercommunal
violence. Credit: Ton Koene
Niger,April 2014 – Ahead of the rainy season, children line up for their first dose of drugs to prevent malaria, a disease transmitted
by mosquitoes.This new preventive strategy – known as ‘seasonal malaria chemoprevention’ – has already saved thousands of
children’s lives. Credit: Juan Carlos Tomasi/MSF
South Sudan, April 2014 – MSF teams unload essential supplies in Bentiu after a major battle led
to tens of thousands of people fleeing their homes for UN camps, where living conditions pose a
serious health risk. Credit: Hosanna Fox/MSF
Around the world with MSF
Bulgaria, May 2014 – Five-year-old Aya Abbas and her three-year-old brother Ala Abbas, from
Syria, have a medical check-up from MSF doctor Rebwar Mustafa in Harmanli refugee camp.
Credit: Alessandro Penso
Uganda, March 2014 – A South Sudanese man is treated by an MSF doctor
in Dzaipi hospital, Adjumani district, where more than 65,000 refugees are
living in overcrowded camps to escape the conflict in their own country.
Credit: Matthias Steinbach
Burkino Faso, April 2014 – In remote Oudalan province,
the only free healthcare available to refugees from Mali is
provided by MSF. Credit: Marie Hortense Koudika
Jordan,April 2014 – An MSF doctor performs surgery. Most of MSF’s
patients in Jordan were wounded in fighting in neighbouring Syria.
Credit: MSF
YOUR SUPPORT
£10.76
pays for a box of 300 surgical gloves
£17.26
pays for a surgical gown
£30.20
pays for a box of 300 surgical masks
£161.41
pays for a basic surgery set of 27 instruments
£
A sick woman is rushed to the hospital where MSF works
in Bossangoa. Credit: Marcus Bleasdale/VII
The violence
affecting Central
African Republic
continues
unabated, with
civilians bearing the
brunt of the clashes between
militias and armed groups.
MSF nurse Alison Criado-
Perez describes what it is like
to work in this conflict zone.
2 April, 2014
I’ve just come back from a bike ride. The
sky is blue and cloudless, the green verges
are splashed with the bright yellow of the first
daffodils. Birds are singing, ponies graze
happily in the fields. Spring is arriving, and all
is tranquil in the peaceful countryside of
Rutland, where I‘m lucky enough to live.
My mind turns to where I will be in just four
days. Bangui, capital of Central African Republic,
and scene for the last few months of the most
horrendous acts of violence. When I came back from
DR Congo just before Christmas, I said I’d done
my last mission with MSF. It was incredibly tough
physically, and I thought that at my age — which
is a secret, but I’ll admit to having my bus pass — I
didn’t think I wanted to put myself through that
again. But I always say going on mission is rather
like having a baby: you forget what an ordeal it was
and just go for it again!
Getting a request to help in such an extreme
situation is a challenge I can’t refuse. Tough it
will be, probably tougher than anything I’ve
done before, but we’ll be providing healthcare
to a terrified and distraught population where
otherwise there would be none.
Which is why I’ll be on the plane to Bangui in a few
days, far from this green and pleasant land, where, in
the lottery of life, I had the good fortune to be born.
9 April, 2014
My natural alarm clock woke me this morning,
as usual, at 5.15: a bird warbling in a mango tree
outside my room. That sounds idyllic, a far cry from
the horrors that are occuring just a kilometre or
so from our house here. As I sit writing on my day
off (in spite of the emergency, we try to have a day
off each week, to recoup our strength for the week
ahead) – the birds are still singing, but their sweet
Gunfire amid
the birdsong sound is interspersed by the rattle of gunfire.
It’s surprising how quickly you get used to an
abnormal situation. As well as the background
of gunshots and shelling, I’m getting used to the
strong military presence, with heavily armoured
cars rolling down the main streets heading to
the flashpoints. Although I was fairly alarmed
on leaving the hospital one afternoon to find the
perimeter wall surrounded by crouching soldiers,
machine-guns at the ready. For a brief second
I thought we were being attacked, but quickly
realised they were protecting a journalist who was
interviewing someone.
I’m also getting used to different classifications
for the MSF statistics. Normally I’m filling
in details of how many cases of malaria,
respiratory tract infections, diarrhoeal diseases
or malnourished children we’re treating; now
I’m classifying the admissions to the emergency
department by wounds from gun shot, grenade
or “arme blanche” – the latter being any other
type of weapon, mostly machetes.
I’ve been here two weeks now, as the nurse/
medical focal point for the hospital MSF started
running on behalf of the Ministry of Health.
Previously a maternity hospital, we have provided
a team to deal with the emergency trauma cases as
well as keeping the maternity department going.
Joy amidst the tragedy
On my first day, our departure to the hospital
was delayed because of an “incident” in a largely
Muslim neighbourhood bordering the hospital.
When we arrived, several people were in the
emergency room being treated for shrapnel
wounds. It seems a young boy had thrown a
grenade.
And so it has continued most days, although this
last week the number of admissions for conflict
trauma has diminished. There are joys among the
tragedies. Belen, one of our doctors, came into
the pharmacy where I was doing the boring but
necessary task of counting stock. “Do you want to
see a miracle?” she asked. Of course I did. I looked
down at the tiny bundle, the 800-gram baby,
who had arrived prematurely. Tiny but alive. This
conflict brings hardship to so many, but delivering
a baby safely can be especially difficult. This
little mite could now be referred to a specialist
paediatric centre run by MSF.
It’s good to have the miracles in the midst of the
ongoing tragedy.
MSF is running 20 projects across Central
African Republic, providing lifesaving
medical care and humanitarian assistance.
Since January, we have treated more than
3,250 people for violence-related injuries,
conducted more than 300,000 outpatient
consultations and treated over 3,000 people
for malaria.
For more information, visit: msf.org.uk/car
WHAT MSF IS DOINGi
Dr Tahir Wissanji changes the dressing on the leg of a 10-year-old boy in MSF’s clinic at Mpoko camp, Bangui. Credit: Christian Nestler
SUDAN
CHAD
S. SUDAN
CENTRAL AFRICAN REPUBLIC
Bangui
Bossangoa
CONGO
DEMOCRATIC REPUBLIC OF CONGO
Bouca
CAMEROON
ADVERTISING FEATURE ADVERTISING FEATURE
5. Médecins Sans Frontières/Doctors Without Borders (MSF) Charity Registration Number 1026588
67-74 Saffron Hill London EC1N 8QX Tel: 44 (0)207 404 6600 Web: www.msf.org.uk
8
Delivering medicine
in a city under siege
In late 2010 and the beginning of
2011, the situation in my country
started to deteriorate. First, there were the
demonstrations and protests in the capital,
Sana’a; then violent clashes broke out all
over the country.
At the time, I was working for MSF and the
Ministry of Health at the HIV clinic in Al-
Gumhuri hospital, the only facility in Sana’a that
provides livesaving antiretroviral (ARV) treatment
to patients suffering from the virus.
Prepared for the worst
It was clear to us that we needed to be prepared
for the worst. With more than 350 patients
receiving livesaving ARV treatment at our
facility, we needed to put a plan in place that
meant we could continue to get drugs to patients
if conflict broke out.
In Yemen, getting treatment for HIV is already
difficult. As a general rule, HIV-positive patients
find getting tested and treated for the illness very
difficult because of the stigma associated with
it. They’ve been misinformed about the disease,
and have lived their whole lives seeing how
HIV-positive people are discriminated against
– even by health workers. Even I personally had
misconceptions around HIV until I trained as a
nurse, and learned the science behind it.
In spring 2011, the fighting intensified and
Sana’a was divided into two sides. Different
armed groups took over sections of the city,
and moving around became extremely difficult.
Clashes around the hospital meant the staff
were trapped inside for three days. The situation
became too dangerous for foreign staff to hang
around – they were all moved to safe houses and
flown out of the country.
‘Without the drugs, our patients
could die’
But most of the Yemeni staff – myself included
– stayed on. Though we could no longer run our
regular activities at Al-Gumhuri, we still needed
to get ARV drugs to the HIV patients, or else
their condition could deteriorate, and they could
even die. So we put our well-laid plans into
action.
In the months leading up to the conflict, the
MSF and Ministry of Health staff had given
special cards to each of our patients. The cards
were a way for patients to get in touch when
they needed their medication delivered, should
we have to suspend our normal activities. These
health cards didn’t have any information on
them that could identify them or me – they had
my phone number on it, and that’s all.
Undercover drop-offs
The patient would call me and give me their
patient number. From that number, I’d know
what kind of drug regimen they were on and
I’d be able to collect the appropriate ARVs
from storage. The patient would then give me
a location, and I’d either take my car to drop
the appropriate ARV medication off there, or
I’d leave it – tucked discreetly into a shopping
bag – wherever they requested. Doing this, I
visited some pretty unusual locations – I once
was asked to leave the drugs in a supermarket;
another time, a photographer’s studio.
Sometimes patients would even come to my
home and collect the drugs that they required;
or I’d pick them up in the street, give them their
drugs while I drove, and then drop them off in
another location so as to avoid putting ourselves
in danger. People would call me day and night;
I had no idea how long this was going to go on
for, so at times it seemed like it would never
end. It didn’t matter to me how it happened,
though. All that mattered is that the sick people
got treated, even while the two sides of the city
were on lockdown.
Scary and stressful
After three months, the active fighting came
to an end, and we were able to resume full
activities in Sana’a. And for all the hard work,
the plan was a success: we were able to reach
all of the 363 patients needing ARV treatment
during the fighting, with 97 percent of them
coming back to us to continue their treatment
after it was over. There were some scary and
stressful times, but I never felt like it was too
much for me. In fact, the patients became like
family to me – I was often the only person they
could trust. I hope there will never again be
unrest like this in my country. But if ever there
is, we’ll be ready.
YEMEN
Abdulbaset Alzamar is a
Yemeni nurse working for
MSF and the Yemeni Ministry
of Health. He talks about his
experience providing live-
saving medicines to HIV
patients as unrest tore the
capital, Sana’a, apart.
YOUR SUPPORT
Conflict, hunger, disease, disaster.
MSF tries to go where we are needed
most. But our staff can only help if they
have training and resources. We can
only provide these if people give to us.
Please support us today.
Phone 0800 408 3894
Visit: www.msf.org.uk/support
Or use the form on page 3
£
HIV is a hidden problem in the Yemeni capital, Sana’a.
Credit: Anna Surinyach/MSF
SUPPORT MAKES OUR WORK POSSIBLE + WE CAN’T OPERATE WITHOUT YOU + YOUR SUPPORT SAVES LIVES + YOUR
Despite a volatile security situation, MSF teams are finding ways to work in Yemen, including with HIV patients, migrants and
people in need of emergency surgical care. Credit: Anna Surinyach/MSF
‘
‘
ADVERTISING FEATURE